|

Awards




















Nothing on this
Beat the Press was written by this civilian editor and consumer
advocate.
Nothing on this
Beat the Press was written by this civilian editor and consumer
advocate.
Nothing on this
Beat the Press was written by this civilian editor and consumer
advocate.
Nothing on this
Beat the Press was written by this civilian editor and consumer
advocate.
Nothing on this
Beat the Press was written by this civilian editor and consumer
advocate. |
 You will find in this section
the latest medical thoughts expressed by the experts
themselves which we feel are of
national importance to all folks. No opinions
expressed were written by this civilian editor.
Note - FDA is a patriotic institution. You will find in this section
the latest medical thoughts expressed by the experts
themselves which we feel are of
national importance to all folks. No opinions
expressed were written by this civilian editor.
Note - FDA is a patriotic institution.
-
FDA announces
comprehensive regulatory plan to shift
trajectory of tobacco-related disease, death
- FDA approves first treatment for
certain types of poor-prognosis acute
myeloid leukemia
- Federal judge enters consent decree
against outsourcing facility Isomeric
Pharmacy Solutions
U.S. District Judge Robert J. Shelby entered a consent
decree of permanent injunction yesterday between the United
States and Isomeric Pharmacy Solutions of Salt Lake City,
Utah, two of the company’s co-owners, William O. Richardson
and Rachael S. Cruz, and chief operating officer Jeffery D.
Brown.
The consent decree prohibits Isomeric, its owners and
chief operating officer from manufacturing, processing,
packing, holding, or distributing drugs until they comply
with the Federal Food, Drug, and Cosmetic Act (FD&C Act) and
its regulations, in addition to other requirements.
According to the complaint for permanent injunction,
Isomeric manufactured and distributed purportedly sterile
drug products, including injectable and ophthalmic drugs
that were adulterated because the drugs were made under
insanitary conditions and in violation of current good
manufacturing practice requirements under the FD&C Act.
Drugs prepared, packed, or held under insanitary conditions
may have been contaminated with filth or otherwise harmful
if given to patients. The complaint also alleges that
Isomeric manufactured and distributed unapproved drugs and
drugs that were misbranded because their labeling did not
bear adequate directions for use.
“Isomeric endangered the public health by manufacturing
injectable drugs under poor conditions that compromised
their required sterility and put patients at risk,” said FDA
Commissioner Scott Gottlieb, M.D. “We will continue taking
strong enforcement actions against compounders who violate
the Drug Quality and Security Act and put patients at risk
by failing to produce sterile drugs in compliance with the
law.”
The FDA most recently inspected Isomeric from Feb. 22 to
March 24, 2017.
Following the FDA inspection, because of
a lack of sterility assurance for its purportedly sterile
drug products, Isomeric agreed to a voluntary nationwide
recall of all lots of
unexpired drug products produced for sterile use and
distributed to patients, providers, hospitals, or clinics
nationwide between Oct. 4, 2016 and Feb. 7, 2017.
Previously, the FDA inspected Isomeric in
August 2015
and observed similar poor
conditions and practices for sterile drug production.
Despite assurances that Isomeric was correcting its
violations, a follow-up inspection in
June 2016 revealed that the
company had not implemented adequate corrective actions.
Following this inspection,
the FDA issued a
warning letter
to Isomeric.
Isomeric initially registered as an
outsourcing facility
in July 2015,
re-registered in December 2015 and January 2017.
The complaint was filed by the U.S. Department of Justice
on behalf of the FDA.
The FDA, an agency within the U.S. Department of Health
and Human Services, protects the public health by assuring
the safety, effectiveness, and security of human and
veterinary drugs, vaccines and other biological products for
human use, and medical devices. The agency also is
responsible for the safety and security of our nation’s food
supply, cosmetics, dietary supplements, products that give
off electronic radiation, and for regulating tobacco
products.
UPDATED 08/07/2015 -
Update includes a corrected
and complete listing of
affected drugs. If there is
contamination in products
intended to be sterile,
patients are at risk of
serious infections which may
be life threatening.
Originally Posted 07/24/2015
If this occurs, the
tip could enter the
patient’s bloodstream. This
could cause serious injury
to the patient and require
additional medical
intervention to retrieve the
tip, or cause death. Posted
08/07/2015
Increased rate of pump
thrombosis, high rate of
stroke, bleeding
complications. Posted
08/05/2015
Cases of PML in two
patients with no prior
exposure to
immunosuppressant drugs.
Posted 08/04/2015
Hospitals and health
care facilities can, in
addition to meticulously
following manufacturer
reprocessing instructions,
take additional steps to
further reduce the risk of
infection. Posted 08/04/2015
Missing a dose of
Hydrochlorothiazide could
result in uncontrolled blood
pressure or swelling caused
by excess fluid (edema).
Posted 07/31/2015
The device could be
accessed remotely through a
hospital’s network. This
could allow an unauthorized
user to control the device
and change the dosage the
pump delivers, which could
lead to over- or
under-infusion of critical
patient therapies. Posted...
ALZHEIMER'S DIAGNOSTIC GUIDELLINES UPDATED FOR
FIRST TIME IN DECADES
For the first time in 27 years, clinical diagnostic criteria for
Alzheimer’s disease dementia have been revised, and research
guidelines for earlier stages of the disease have been characterized
to reflect a deeper understanding of the disorder. The National
Institute on Aging/Alzheimer’s Association Diagnostic Guidelines for
Alzheimer’s Disease outline some new approaches for clinicians and
provide scientists with more advanced guidelines for moving forward
with research on diagnosis and treatments.
They mark a major change in how experts think about and study
Alzheimer’s disease. Development of the new guidelines was led by
the National Institutes of Health and the Alzheimer’s Association.
The original 1984 criteria were the first to address the disease and
described only later stages, when symptoms of dementia are already
evident. The updated guidelines cover the full spectrum of the
disease as it gradually changes over many years. They describe the
earliest preclinical stages of the disease, mild cognitive
impairment, and dementia due to Alzheimer’s pathology. Importantly,
the guidelines now address the use of imaging and biomarkers in
blood and spinal fluid that may help determine whether changes in
the brain and those in body fluids are due to Alzheimer’s disease.
Biomarkers are increasingly employed in the research setting to
detect onset of the disease and to track progression, but cannot yet
be used routinely in clinical diagnosis without further testing and
validation.
CDC AMERICA AGEING IN POVERTY
FDA warns
public of continued extortion scam by FDA
impersonators
FDA NEWS RELEASE
For Immediate Release: Jan.
7, 2011
Media Inquiries: Christopher
Kelly, 301-796-4676 christopher.kelly@fda.hhs.gov
Consumer Inquiries:
888-INFO-FDA
The U.S. Food and Drug Administration is
warning the public about criminals posing as
FDA special agents and other law enforcement
personnel as part of a continued
international extortion scam.
The criminals call the victims -- who in
most cases previously purchased drugs over
the Internet or via "telepharmacies" -- and
identify themselves as FDA special agents or
other law enforcement officials. The
criminals inform the victims that purchasing
drugs over the Internet or the telephone is
illegal, and that law enforcement action
will be pursued unless a fine or fee ranging
from $100 to $250,000 is paid. Victims often
also have fraudulent transactions placed
against their credit cards.
The criminals always request the money be
sent by wire transfer to a designated
location, usually in the
Dominican Republic.
If victims refuse to send money, they are
often threatened with a search of their
property, arrest, deportation, physical harm
and/or incarceration.
"Impersonating an FDA official is a
violation of federal law," said Dara
Corrigan, the FDA’s associate commissioner
for regulatory affairs. “FDA special agents
and other law enforcement officials are not
authorized to impose or collect criminal
fines. Only a court can take such action.”
In most instances, victims of
extortion-related calls have also received
telephone solicitations for additional
pharmaceutical purchases from other possibly
related, illegal entities located overseas.
The extortionists use customer lists
complete with extensive personal information
provided through previous purchase
transactions. These include names,
addresses, telephone numbers, Social
Security numbers, dates of birth, purchase
histories and credit card account numbers.
Typically, these criminals use telephone
numbers that change constantly and make it
appear as though their calls originate in
the
United States.
No known victim has been approached in
person by a law enforcement impersonator
associated with this scheme.
The FDA’s Office of Criminal Investigations,
with the U.S. Drug Enforcement
Administration, and the U.S. Immigrations
and Customs Enforcement, Homeland Security
Investigations, with the support of various
U.S. Attorneys, are pursuing multiple
national and international criminal
investigations.
Arrests have been made and additional
prosecutions are pending; however, the
scheme is likely to continue. The FDA has
issued similar warnings in the past:
§
FDA Warns Public of Extortion Scam by FDA
Impersonators
(11/12/2008)
§
FDA
Warns Public of Continued Extortion Scam by
FDA Impersonators
(12/29/2009)
Victims of this scheme who have suffered
monetary loss through the payment of funds
in response to an extortion call from a
person purporting to be an FDA or other law
enforcement official regarding illegal
pharmaceutical transactions may obtain a
victim questionnaire by contacting the
FDA’s Office of Criminal Investigations
and clicking “Report Suspected Criminal
Activity.”
Anyone receiving a
purported official document on agency
letterhead may verify its authenticity by
contacting that organization directly via
a publicly available phone number.
Additionally, all federal agencies use email
addresses with a “gov” email extension.
The
FDA also reminds consumers that
pharmaceutical products offered online and
by telephone by sources of unknown origin
can pose a substantial health risk. Products
recovered during this investigation that
were purchased from online or telephone
sources have been found to contain trace
amounts of heroin, other undisclosed and
potentially harmful active pharmaceutical
ingredients, or no active ingredient at all.
Purchases should only be made from licensed
pharmacies located in the
United States.
In addition to the increased risk of
purchasing unsafe and ineffective drugs from
Web sites operating outside the law,
personal data may be compromised.
For more on unlawful drug sales on the
Internet, see
Protecting Yourself.
Questions and Answers
How did these people
obtain my information?
They likely obtained the victim’s
information based on a previous online or
telepharmacy transaction, or from a
submitted medical questionnaire. These
instances could have occurred years ago,
with personal information now on customer
lists trafficked by these criminal groups.
These customer lists can contain tens
of thousands of names and a substantial
amount of self-reported data provided by
consumers during previous transactions.
Typically, victims are being
contacted by multiple unrelated groups,
often for different purposes. (extortion,
selling illegal pharmaceuticals, etc.)
How do I make the
calls stop?
The extorters, just like the majority of
telephone solicitors for illegal
prescription medication, are based overseas
and use voice over internet protocol (VOIP)
telephone numbers, most commonly “Magic
Jack”. These
services provide the extorters with the
flexibility to constantly change their phone
numbers and select ones with
U.S. area codes.
If the victims
change whatever number(s) were used
to contact them, and do not engage in any
additional risky pharmaceutical
transactions, the threatening phone calls
and associated telephone solicitations for
pharmaceuticals should cease.
What proactive steps
can victims take?
Individuals who purchase medication online
or via tele-pharmacies are frequently
victims of credit card fraud, since this is
how the medication is often purchased.
Victims may want to consider alerting
their applicable financial institutions to
ensure that identity theft has not occurred.
Why is FDA only asking
victims who have lost money to contact the
agency?
The most effective way to track these
criminals is to investigate the permanent
record established when money transfers take
place.
Have individuals been
arrested?
Yes.
However,
this scheme will likely not be eradicated
and instead will continue to evolve.
For example, the extorters now
occasionally reference other countries, such
as
Costa Rica,
instead of the DR, as means to avoid all of
the publicity regarding this scheme.
Am I going to be able
to get my money back?
In almost all
instances victims will not be able to recoup
losses. Multiple
criminal groups employ this scheme,
principally from overseas, and large
monetary seizures are not anticipated.
Am I in danger?
In terms of physical danger, no victim has
ever been approached in person, and the vast
majority of these callers, regardless of
their intent, are based overseas.
Their use of “police-type scanners”,
law enforcement language and fictitious
documents are attempts at a false sense of
legitimacy. Extorters also occasionally
reference cars parked on a victim’s street
-- information that can be obtained online
at various Web sites, as a way to frighten
individuals into believing the extorters are
near their residence.
If an individual feels threatened for
his or her personal safety, immediately
contact the appropriate local enforcement
agency.
Is it possible that
these callers are part of some “secret”
investigative group, and FDA is just not
aware of it?
No.
Law
enforcement officials from both the
U.S. and the
Dominican Republic
are pursuing these criminals.
More information regarding this
scheme is available on FDA and DEA Web
sites, or through online searches.
Extradition proceedings
between countries require close
cooperation and often a formal treaty, and
this often takes an extended period of time
to complete
CDC Releases 2011 National Diabetes Fact Sheet
According to the Centers for
Disease Control and Prevention’s (CDC) new estimates, the
number of Americans with diabetes has risen to 25.8 million.
About 27 percent of those with diabetes – 7 million
Americans – do not know they have the disease. 1 in 3 U.S.
adults is at high risk of developing type 2 diabetes.
Further, an estimated 79 million U.S. adults have
prediabetes, a condition in which blood sugar levels are
higher than normal, but not high enough to be considered
diabetes. Prediabetes raises a person’s risk of type 2
diabetes, heart disease and stroke, and affects 35 percent
of adults aged 20 years and older.
New Dietary Guidelines Have Been Released by the
U.S. Department of Health and Human Services and the
U.S. Department of Agriculture
On January 31, 2011, the
Secretary of Agriculture, Tom
Vilsack and the Secretary of the
Department of Health and Human
Services, Kathleen Sebelius
announced the release of the
2010 Dietary Guidelines for
Americans, the federal
government’s evidence-based
guidance to promote health,
reduce the risk of chronic
diseases, and reduce the
prevalence of overweight and
obesity through improved
nutrition and physical activity.
The new 2010 Dietary Guidelines
for Americans focus on balancing
calories with physical activity,
and encourage Americans to
consume more healthy foods like
vegetables, fruits, whole
grains, fat-free and low-fat
dairy products and seafood and
to consume less sodium,
saturated and trans fats, added
sugars, and refined grains.
“Helping Americans incorporate
these guidelines into their
everyday lives is important to
improving the overall health of
the American people,” said HHS
Secretary Sebelius. “The new
Dietary Guidelines provide
concrete action steps to help
people live healthier, more
physically active and longer
lives.”
USDA and HHS have conducted this
latest review of the scientific
literature, and have developed
and issued the 7th edition of
the Dietary Guidelines for
Americans in a joint effort that
is mandated by Congress. The
Guidelines form the basis of
federal nutrition policy, as
well as Federal nutrition
assistance programs such as
congregate and home delivered
meals of the Older Americans Act
Nutrition Program and nutrition
advice provided by health care
professionals.
FDA:
U.S. Marshals seize food products at
Tennessee company
FDA acts to prevent
distribution of food from
rodent-infested facility
U.S.
Marshals today seized about $200,000
worth of food products from Bedford
Cheese Store Inc. in Shelbyville,
Tenn., after U.S. Food and Drug
Administration investigators found
evidence of rodents throughout the
company’s facility.
An FDA inspection found rodent
feces, rodent hair, rodent nesting
material, and building defects that
could allow rodents and other pests
to enter food storage areas and
other areas that apparently
contributed to the infestation.
Products seized at Bedford Cheese
included cheese, frozen foods,
pastas, salad dressings, prepared
salads, soups, and various bulk
ingredients. The products are
adulterated under the Federal Food,
Drug and Cosmetic Act because they
have been held under unsanitary
conditions and may have become
contaminated with filth.
“The violations at Bedford Cheese
are widespread and significant,”
said Dara A. Corrigan, the FDA’s
associate commissioner for
regulatory affairs. “This
enforcement action was taken because
the company failed to provide
adequate safeguards to ensure that
products they produce or hold for
sale remain free of contamination.”
In a written response to the FDA
following the inspection, Bedford
Cheese committed to cleaning up its
facility. However, the company
failed to complete all corrective
actions, including the development
and implementation of a pest control
plan to rid the facility of the
active rodent infestation.
FDA: Advanced genomic test helps
trace sources of foodborne illness outbreak
Next-generation sequencing provides important clues to
traceback investigation
FDA scientists successfully used a new genome
sequencing test to retrospectively examine a 2009-10
foodborne illness outbreak to help trace the source
of the infection.A Salmonella Montevideo outbreak
that began early in 2010 was linked to spice rubs on
certain salamis and sickened nearly 300 people in 44
states and the District of Columbia.
Field investigators collected samples of the
suspect product to find the source of the
contamination. However, conventional laboratory
testing methods could not distinguish between the
outbreak involving spiced meat and certain previous
Salmonella contamination events.
FDA analysts then turned to next-generation
sequencing (NGS) to test 35 samples suspected of
being contaminated with the Salmonella strain. The
samples came from suppliers, consumers who became
ill and a variety of food sources from a broad range
of places and times.
Test results showed a recent common origin of the
outbreak strain – a single food facility. The
results also indicated a single source: a spiced
meat rub.
The findings supported the information gathered
in the field phase of the investigation and suggest
an important role for this novel tool in augmenting
future outbreak investigations.
or more information:
Identification of a Salmonellosis Outbreak by
Means of Molecular Sequencing
New England Journal of Medicine,
http://www.nejm.org/doi/full/10.1056/NEJMc1100443
Salmonella Montevideo Outbreak: FDA News Release
http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/2010/ucm204917.htm
Salmonella Montevideo Outbreak: CDC Investigation
Update
http://www.cdc.gov/salmonella/montevideo/index.html
FDA approves product
to prevent bleeding in people with rare genetic
defect
Corifact is 1st treatment for
congenital Factor XIII Deficiency
The U.S. Food and Drug Administration today
approved Corifact, the first product intended to
prevent bleeding in people with the rare genetic
defect congenital Factor XIII deficiency.
Patients with congenital Factor XIII deficiency
don’t make enough Factor XIII, a substance that
circulates in the blood and is important for normal
clotting. Without treatment, people with the
condition are at risk for life-threatening bleeding.
Congenital Factor XIII deficiency is rare and
affects 1 out of every 3 million to 5 million people
in the United States. The deficiency may lead to
soft tissue bruising, mucosal bleeding and fatal
intracranial bleeding. Newborns with Factor XIII
deficiency may have umbilical cord bleeding.
“This product helps fill an important need,” said
Karen Midthun, M.D., director of the FDA’s Center
for Biologics Evaluation and Research.
Corifact received orphan-drug designation by the
FDA because it is intended for use in a rare disease
or condition. It was approved for marketing under
the FDA's accelerated approval regulations that
require an on-going study to demonstrate that
patients actually receive the clinical benefit
predicted by the data obtained so far.
The FDA approved Corifact based on results of a
clinical study of 14 people, including children,
with congenital Factor XIII deficiency. The most
common side effects observed were hypersensitivity
reactions (allergy, rash, pruritus, and erythema),
chills, fever, arthralgia, headache, elevated
thrombin-antithrombin levels, and an increase in
liver (hepatic) enzymes.
Corifact is made from the pooled plasma of
healthy donors. People receiving Corifact may
develop antibodies against Factor XIII that may make
the product ineffective. It potentially can cause
adverse events from abnormal clotting if doses
higher than the labeled dose are given to patients.
Corifact is manufactured by CSL Behring of
Marburg, Germany.
For more information:
CBER Product Approvals
FDA
warns against certain uses of asthma
drug terbutaline for preterm labor
Certain uses could lead
to maternal heart problems and deathThe U.S. Food and Drug
Administration is warning that
terbutaline administered by
injection or through an infusion
pump should not be used in pregnant
women for prevention or prolonged
(beyond 48-72 hours) treatment of
preterm labor due to the potential
for serious maternal heart problems
and death. In addition, oral
terbutaline tablets should not be
used for prevention or treatment of
preterm labor. The FDA is requiring
the addition of a Boxed Warning and
Contraindication to the drug
prescribing information (labeling)
to warn against these uses.
Terbutaline is FDA-approved to
prevent and treat narrowing of the
airways (bronchospasm) associated
with asthma, bronchitis, and
emphysema. The drug is used
off-label for obstetric purposes,
including treating preterm labor and
treating uterine hyperstimulation.
Terbutaline has also been used in an
attempt to prevent recurrent preterm
labor. There is no evidence,
however, that use of terbutaline to
prevent preterm labor improves
infant outcomes. Serious adverse
events, including maternal deaths,
have been reported with such use in
pregnant patients.
“Women should be aware that
serious and sometimes fatal side
effects have been reported after
prolonged use of terbutaline in
pregnant women,” said Scott Monroe,
M.D., director of FDA’s Division of
Reproductive and Urologic Products.
“It is important for patients and
health care professionals to
consider all the potential risks and
known benefits of any drug before
deciding on its use.”
The FDA is aware that
administration of terbutaline by
injection to pregnant women is used
in hospital settings in certain
urgent situations. The FDA warning
relates to safety concerns about the
prolonged use of terbutaline
injection beyond 48-72 hours, and
against any use of oral terbutaline
in pregnant women for prevention or
treatment of preterm labor.
The decision to require a Boxed
Warning and Contraindication is
based on the FDA’s review of
post-market safety reports of heart
problems and even death associated
with terbutaline use for obstetric
indications, as well as data from
medical literature documenting the
lack of safety and effectiveness of
terbutaline for preventing preterm
labor, and animal data suggesting
potential risks. Based on this
information, the FDA concluded that
the risk of serious adverse events
outweighs any potential benefit to
pregnant patients for either
prolonged use of terbutaline
injection beyond 48-72 hours or use
of oral terbutaline for prevention
or treatment of preterm labor.
These changes to the drug
labeling are consistent with
statements from the American College
of Obstetricians and Gynecologists
discouraging use of terbutaline for
preventing preterm labor.
There are multiple generic
versions of terbutaline oral tablets
and injectable formulations
available. The brand name products
were previously discontinued by the
companies that made them.
The FDA encourages patients to
talk to their health care
professional if they have concerns
about any treatment they are
receiving. Patients and health care
professionals should report any side
effects from the use of terbutaline
to the FDA’s MedWatch adverse event
reporting program at
www.fda.gov/MedWatch.
For more information:
U.S. Marshals seize
Auralgan Otic
Solution
Product
is not FDA-approvedU.S. Marshals, at
the request of the
U.S. Food and Drug
Administration
yesterday, seized
all lots of Auralgan
Otic Solution, a
prescription drug
used to treat pain
and inflammation
associated with ear
infections, from
Integrated
Commercialization
Solutions Inc. (ICS)
in Brooks, Ky.
Auralgan is
manufactured for
Deston Therapeutics,
located in Chapel
Hill, N.C., and is
warehoused at ICS.
Deston’s sale of
the product in the
United States
violates federal law
because the product
does not have FDA
approval and its
labeling does not
include adequate
directions for use.
The value of the
products seized is
estimated to be
$16.5 million.
“The FDA is
committed to taking
enforcement action
against companies
marketing drugs that
do not meet federal
standards for
safety,
effectiveness, and
quality,” said
Deborah M. Autor,
director of the
Office of Compliance
in the FDA’s Center
for Drug Evaluation
and Research. “We
will remain vigilant
in our efforts to
protect consumers
from unapproved
products.”
On Feb. 5, 2010,
the FDA issued a
Warning Letter to
Deston, citing the
company for
distributing
unapproved new drugs
and misbranded
drugs. The FDA also
warned Deston that
Auralgan was an
unapproved new drug
in April, June, and
September 2010, and
the company
continued
distributing the
drug in violation of
the Federal Food,
Drug, and Cosmetic
Act.
Today’s action is
part of the FDA’s
Unapproved Drugs
Initiative,
established in 2006
to get unapproved
drugs either
approved or off the
market.
For more
information:
February 5, 2010
Warning Letter to
Deston Therapeutics,
LLC
Unapproved Drugs:
Drugs Marketed in
the United States
That Do Not Have
Required FDA
Approval
FDA seeks to invest
in foodborne illness
prevention, medical
product safety and
countermeasures
$4.3
billion request
reflects a 33
percent increase
from FY 2010 enacted
budget
The U.S. Food and Drug Administration is requesting a budget of
$4.3 billion to
protect and promote
the public health as
part of the
President’s fiscal
year (FY) 2012
budget — a 33
percent increase
over the FDA enacted
budget for FY 2010.
The FY 2012 request
covers the period of
Oct. 1, 2011,
through Sept. 30,
2012.
“FDA protects and
promotes the health
of all Americans
through every stage
of life,” said
Margaret A. Hamburg,
M.D., commissioner
of food and drugs.
“The breadth of this
mandate means that
FDA responsibilities
continue to grow.
The new budget
contains new
resources so that
FDA can fulfill its
growing
responsibilities to
the American
public.”
The FDA 2012
budget proposes four
critical initiatives
and increases:
- Transforming
Food Safety and
Nutrition ($324
million)
Initiative: With
this increase,
FDA will begin
to implement the
landmark Food
Safety
Modernization
Act and also
empower
Americans to
make healthier
food choices.
FDA will
establish a
prevention-focused
food safety
system and
leverage the
valuable work of
FDA’s state and
local food
safety partners.
The result will
be a stronger,
more reliable
food safety
system to
protect American
consumers. FDA
will also
empower
Americans to
make more
healthful food
choices through
menu and vending
machine
labeling.
- Advancing
Medical
Countermeasures
($70 million)
Initiative: This
increase will
ensure that FDA
can support the
development of
medical
countermeasures
(MCMs) to
respond to
serious national
security threats
– chemical,
biological,
radiological and
nuclear threats,
as well as
naturally
emerging
diseases such as
pandemic
influenza. With
this initiative,
FDA will enhance
its review of
countermeasures
and develop and
apply new tools
and standards to
speed the
development of
MCMs. To improve
public health
response, FDA
will also
modernize the
legal,
regulatory and
policy framework
that governs
development and
availability of
MCMs.
- Protecting
Patients
Initiative ($124
million): With
this increase,
FDA will develop
a pathway for
approving
biosimilars,
which are
biological drugs
shown to be
highly similar
to, and without
clinically
meaningful
differences
with, an
FDA-approved
reference
biological
product. Such
biosimilars may
also be shown to
be
interchangeable
with the
FDA-approved
reference
biological
product. These
biosimilars
offer the
potential of
significant
savings for
government and
private sector
healthcare
systems that
provide care to
millions of
Americans. The
Protecting
Patients
Initiative also
strengthens FDA
efforts to
modernize and
improve safety
throughout the
supply chain of
medical
products, and it
contains other
resources to
assure the
safety of
medical
products.
- Regulatory
Science and
Facilities
Initiative ($49
Million): This
request will
allow FDA to
strengthen its
core regulatory
scientific
capacity that
support all
elements of the
FDA mission.
This initiative
will help
harness advances
in science and
technology to
modernize and
streamline the
regulatory
pathway and
improve the
review and
approval process
for products
relying on new
and emerging
technologies
that offer
promising new
opportunities to
diagnose, treat,
cure and prevent
disease.
For more
information:
The President’s FY
2012 budget for the
FDA
http://www.hhs.gov/budget/
Food Safety
Modernization Act:
Putting the Focus on
Prevention
http://www.foodsafety.gov/news/fsma.html
FDA
finalizes regulation for certain software,
hardware used with medical devices
Rule provides more predictable
path to market
Today, the FDA
announced a final
rule that provides a
less-burdensome path
to market for
certain hardware and
software products
used with medical
devices. The rule
classifies these
products, known as
Medical Device Data
Systems or MDDS, as
Class I or low-risk
devices, making them
exempt from
premarket review but
still subject to
quality standards. “This rule is a
common-sense
regulatory approach
that provides
clarity and
predictability for
manufacturers of
these data systems,”
said Jeffrey Shuren,
M.D., director of
the Center for
Devices and
Radiological Health.
“This shows our
flexibility in
applying regulations
for medical device
data systems that
are not overly
burdensome for
manufacturers but
continue to assure
that data stored,
transferred or
displayed on these
systems remain
reliable.”
Medical Device
Data Systems are
off-the-shelf or
custom hardware or
software products
used alone or in
combination that
display unaltered
medical device data,
or transfer, store
or convert medical
device data for
future use, in
accordance with a
preset
specification.
Examples of MDDS
products include:
devices that collect
and store data from
a blood pressure
cuff for future use
or that transfer
thermometer readings
to be displayed at a
nursing station for
future use.
Prior to this
rule, first proposed
in 2008, FDA
considered these
devices to be either
Class III (or
high-risk) devices
requiring premarket
approval or
accessories to an
existing medical
device.
By
down-classifying
these devices into
Class I, the FDA is
exempting all
manufacturers of
MDDS from premarket
notification and
applying the level
of regulation
reserved for low
risk devices.
Moreover, these
manufacturers must
comply with all
Class I requirements
including
registering with the
FDA, listing their
MDDS products,
reporting adverse
events and complying
with FDA’s Quality
Systems regulation,
a basic system of
manufacturing and
design controls
that, among other
things, will ensure
manufacturers test
their products
before marketing
them.
The rule also
levels the playing
field for medical
device
manufacturers.
Information
technology companies
that design, install
or market these
systems, and
hospitals that
develop them in
their facilities,
must follow Class I
requirements as
well.
The Medical
Device Data Systems
rule will be
published in the
Federal Register
tomorrow and is
available for
advanced viewing
today.
For more
information
Medical Device Data
Systems
- EFFECTIVENESS OF VARIOUS INTERVENTIONS FOR ACUTE
OTITIS EXTERNA
Authors Kaushik
Vivek, Malik Tass, Saeed Shakeel R
Review Group Cochrane Ear, Nose and Throat Disorders
Group
Abstract Acute otitis externa is an inflammatory
condition of the ear canal, with or without infection. Symptoms
include ear discomfort, itchiness, discharge and impaired hearing.
It is also known as 'swimmer's ear' and can usually be treated
successfully with a course of ear drops.
Objectives:
To assess the effectiveness of interventions for acute otitis
externa.
Search strategy:
Our search for published and unpublished trials included the
Cochrane Ear, Nose and Throat Disorders Group Trials Register;
CENTRAL; PubMed; EMBASE; CINAHL; Web of Science; BIOSIS Previews;
Cambridge Scientific Abstracts; mRCT and additional sources. The
date of the most recent search was 6 January 2009.
Selection criteria:
Randomised controlled trials evaluating ear cleaning, topical
medication or systemic therapy in the treatment of acute otitis
externa were eligible.We excluded complicated acute otitis externa;
otitis externa secondary to otitis media or chronic suppurative
otitis media; chronic otitis externa; fungal otitis externa (otomycosis);
eczematous otitis externa; viral otitis externa and furunculosis.
Data collection and analysis:
Two authors assessed eligibility and quality.
Main results:
Nineteen randomised controlled trials with a total of 3382
participants were included. Three meta-analyses were possible. The
overall quality of studies was low.
Topical antimicrobials containing steroids were significantly more
effective than placebo drops: OR 11 (95% CI 2.00 to 60.57; one
trial). In general, no clinically
meaningful differences were noted in clinical cure rates between the
various topical interventions reviewed. One notable exception
involved a trial of high quality which showed that acetic acid was
significantly less effective when compared with antibiotic/steroid
drops in terms of cure rate at two and three weeks (OR 0.29 (95% CI
0.13 to 0.62) and OR 0.25 (95% CI 0.11 to 0.58) respectively).
One trial of low quality comparing quinolone with non-quinolone
antibiotics did not find any difference in clinical cure rate.
No trials evaluated the effectiveness of ear cleaning.
Only two trials evaluated steroid-only drops. One trial of
low quality suggested no significant difference between steroid and
antibiotic/steroid but did not report the magnitude or precision of
the result. Another trial of moderate quality comparing an oral
antihistamine with topical steroid against topical steroid alone
found that cure rates in both groups were high and comparable (100%
(15/15) and 94% (14/15) respectively at three weeks).
Authors' conclusions:
There is a paucity of high quality trials evaluating
interventions for acute otitis externa. The results of this
systematic review are largely based on odds ratios calculated from
single trials, most of which have very broad 95% confidence
intervals because of small to modest sample sizes. The findings may
not be wholly generalisable to primary care for a variety of
reasons; only two of the 19 trials included in the review were
conducted in a primary care population setting, and in 11 of the 19
trials ear cleaning formed part of the treatment (an intervention
unlikely to be available in primary care). Despite these
reservations, some meaningful conclusions can be drawn from the
evidence available: Topical
treatments alone, as distinct from systemic ones, are effective for
uncomplicated acute otitis externa. In most cases the choice of
topical intervention does not appear to influence the therapeutic
outcome significantly. Any observed differences in efficacy were
usually minor and not consistently present at each follow-up visit.
Acetic acid was effective and comparable to antibiotic/steroid at
week 1. However, when treatment needed to be extended beyond this
point it was less effective. In addition, patient symptoms lasted
two days longer in the acetic acid group compared to
antibiotic/steroid. The evidence for
steroid-only drops is very limited and as yet not robust enough to
allow us to reach a conclusion or provide recommendations. Further
investigation is needed. Given that
most topical treatments are equally effective, it would appear that
in most cases the preferred choice of topical treatment may be
determined by other factors, such as risk of ototoxicity, risk of
contact sensitivity, risk of developing resistance, availability,
cost and dosing schedule. Factors such as speed of healing and pain
relief are yet to be determined for many topical treatments and may
also influence this decision.
Patients prescribed antibiotic/steroid drops can expect their
symptoms to last for approximately six days after treatment has
begun. Although patients are usually treated with topical medication
for seven to 10 days it is apparent that this will undertreat some
patients and overtreat others. It may be more useful when
prescribing ear drops to instruct patients to use them for at least
a week. If they have symptoms beyond the first week they should
continue the drops until their symptoms resolve (and possibly for a
few days after), for a maximum of a further seven days. Patients
with persisting symptoms beyond two weeks should be considered
treatment failures and alternative management initiated.
Implications High quality level 1 evidence regarding
interventions for acute otitis externa is sparse. The comparison
categories studied in this review mostly contain single trials only.
Only three meta-analyses were possible. Results are largely based on
odds ratios calculated from single trials, most of which have very
broad 95% confidence intervals because of small to modest sample
sizes. A number of significant results have 95% confidence intervals
whose limits approach 1.0, suggesting that negligible differences
cannot be excluded. A number of recent trials report results using P
values that do not allow the magnitude or precision of the results
to be evaluated, and as a result any findings merit cautious
interpretation. The findings of this systematic review may not be
wholly generalisable to primary care for a variety of reasons; only
two of the 19 trials included in the review were conducted in a
primary care population setting, and 11 of the 19 trials had ear
cleaning as part of the treatment. Having said all of this, a few
salient points can be made from the evidence available:Topical
treatments alone are effective for uncomplicated acute otitis
externa. Additional oral antibiotics are not required.In most cases
the choice of topical intervention does not appear to influence the
therapeutic outcome significantly. Any observable differences in
efficacy were minor and not consistently present at every assessment
point.Evidence from one trial (Sabater 1996) of low quality found no
difference in clinical efficacy between quinolone and non-quinolone
drops. Quinolones are more expensive than non-quinolones. This
finding may influence their use in cost-driven and resource-poor
settings. If treatment needs to be
extended beyond one week acetic acid alone appears to perform less
well when compared against other topical treatments. One high
quality trial (van Balen 2003) compared acetic acid with
antibiotic/steroid drops; although the cure rate was comparable at
day seven to nine it was poorer in the acetic acid group at weeks
two and three. A separate trial, of low quality, showed that acetic
acid spray had a poorer cure rate than acetic
acid/antibiotic/steroid spray at two and four weeks (Slack 1987).
Acetic acid is available in many countries as a non-prescription
remedy at low-cost, in both drop and spray form. The manufacturer
recommends using it for a maximum of seven days. The results from
van Balen 2003 support their use for this duration. However, their
study also showed that symptoms were more prolonged in the acetic
acid group (eight days versus six days in the antibiotic/steroid
group); this may influence the decision to use acetic acid in
primary care.There is some evidence which indicates that patients
treated with topical antibiotic containing steroid benefit from
reduced swelling (Mosges 2008), severe redness, secretion and
analgesic consumption (Mosges 2007) compared to their non-steroid
counterpart. There is a suggestion that high-potency steroids may be
more effective than low-potency steroids (in terms of severe pain,
inflammation and swelling) (Roland 2007). Further investigation is
required.Evidence from one low quality trial (Masood 2008) suggests
a glycerine-ichthammol medicated wick may provide better pain relief
in early severe acute otitis externa than a triamcinolone/gramicidin/neomycin/nystatin
medicated wick, but the magnitude or precision of effect has yet to
be established. The effectiveness of
ear cleaning is unknown. The evidence for the efficacy of
steroid-only drops is scant and has not been fully established.
Further investigation is warranted in order to quantify the effects
of both these interventions fully.
In general, given the apparent parity in clinical efficacy of
topical interventions used to treat acute otitis externa, other
factors such as cost, availability, dosing regimen, risk of contact
sensitivity, risk of resistance and risk of ototoxicity may
determine the choice of therapy. Parameters such as speed of healing
and pain relief are yet to be determined for many topical treatments
and may also influence this decision.
Patients prescribed antibiotic/steroid drops can expect their
symptoms to last for approximately six days after treatment has
begun. Patients are usually treated for seven to 10 days, although
it is apparent that they are cured at different time points. It may
be more useful when prescribing ear drops to instruct patients to
use them for at least a week. If they have symptoms beyond the first
week they should continue the drops until their symptoms resolve
(and possibly for a few days after) for a maximum of a further seven
days. Patients with symptoms beyond two weeks should be considered
treatment failures and alternative management initiated.
Citation Kaushik V, Malik T, Saeed SR. Interventions
for acute otitis externa. Cochrane Database of Systematic Reviews
2010, Issue 1. Art. No.: CD004740. DOI:
10.1002/14651858.CD004740.pub2.
- IN BREAST
CANCER SURVIVORS, ASPIRIN MAY DECREASE RISK OF DISTANT RECURRENCE
AND BREAST CANCER-RELATED DEATH
Summary "Among women living at least
1 year after a breast cancer diagnosis, aspirin use was associated
with a decreased risk of distant recurrence and breast cancer
death."Basis for Study "Animal and in vitro studies
suggest that aspirin may inhibit breast cancer metastasis." This
prospective study explored whether aspirin use reduces the risk of
death from breast cancer and distant recurrence.
Detailed Summary of Study Breast cancer recurrence
and death were tracked in 4,164 breast cancer patients who were
participants in the Nurses’ Health Study, and rates were compared
based on the number of days per week that the patients took aspirin.
Results/Body Compared to women who did not take
aspirin, adjusted relative risks for breast cancer-related death was
1.07 for women who took aspirin 1 day/week, 0.29 for 2 to 5
days/week, and 0.36 for 6 or 7 days/week. Corresponding figures for
distant recurrence were 0.91, 0.40 and 0.57.
Sources & Other Links Holmes MD, Chen WY, Li L,
Hertzmark E, Spiegelman D, Hankinson SE.
Aspirin intake and survival after breast cancer.
J Clin Oncol. 2010 Feb 16. [Epub
ahead of print]
-
STROKE PATIENTS FACE A HIGHER RISK OF RECURRENT
STROKE, MYOCARDIAL INFARCTION OR DEATH
Summary This study of stroke
patients in South Carolina found that over the next 4 years they had
a higher risk of recurrent stroke, myocardial infarction (MI) or
death. “These finding suggest there is room for further improvement
in secondary stroke prevention in South Carolina.”Basis for
Study This study determined the risk of recurrent stroke,
MI or death in stroke patients.
Detailed Summary of Study The incidence of recurrent
stroke, MI and all-cause death was tracked in 10,399 patients who
were hospitalized for a stroke in 2002. Follow-up was through 2006.
Results/Body Cumulative risk at 1 month, 6 months, 1
year, 2 years, 3 years and 4 years was 1.8%, 5.0%, 8.0%, 12.1%,
15.2%, and 18.1% for recurrent stroke; 0.3%, 1.0%, 2.1%, 3.7%, 5.0%,
and 6.2% for MI; and 14.6%, 20.6%, 24.5%, 30.9%, 36.2%, and 41.3%
for all-cause death. The combined risk for recurrent stroke, MI, or
vascular death was 13.6%, 19.5%, 24.7%, 31.6%, 36.8%, and 41.3%. The
combined risk for recurrent stroke, MI or death was slightly higher
for older patients (hazard ratio 1.38) and for African-Americans
(1.12).
Sources & Other Links Feng W, Hendry RM, Adams RJ.
Risk of recurrent stroke, myocardial infarction, or death in
hospitalized stroke patients. Neurology.
2010 Feb 16;74(7):588-93.
-
INCREASED CHD RISK WITH ESTROGEN PLUS PROGESTIN THERAPY IS
LIMITED TO INITIAL FEW YEARS OF USE
Summary In postmenopausal women, the
increased coronary heart disease risk produced by estrogen plus
progestin therapy decreases only after 6 years of useBasis for
Study “Estrogen plus progestin therapy increases the risk
for coronary heart disease (CHD) in postmenopausal women. However,
this increased risk might be limited to the first years of use and
to women who start therapy late in menopause.” This study was part
of the Women’s Health Initiative.
Detailed Summary of Study The authors traced the CHD
risk in 16,608 women who had been randomized to receive either no
hormone therapy or estrogen plus progestin therapy. The influence of
the duration of hormone use and the timing of use (years since
menopause) was analyzed.
Results/Body Women who used estrogen plus progestin
therapy continuously had a hazard ratio of developing CHD of 2.36
for the first 2 years and 1.69 for the first 8 years, compared to
women who did not take hormones. Corresponding figures were 1.29 and
0.64 for women within 10 years after menopause. “The CHD-free
survival curves for continuous use and no use of estrogen plus
progestin crossed at about 6 years.”
Sources & Other Links Toh S, Hernández-Díaz S, Logan
R, Rossouw JE, Hernán MA.Coronary
heart disease in postmenopausal recipients of estrogen plus
progestin therapy: does the increased risk ever disappear? A
randomized trial. Ann Intern Med.
2010 Feb 16;152(4):211-7.
-
META-ANALYSIS FINDS STATIN USE SEEMS JUSTIFIED DESPITE SLIGHT
INCREASE IN RISK OF DIABETES
Summary This meta-analysis found
that although statin use may be associated with a modest increase in
the risk of diabetes, its effectiveness at reducing the risk of
coronary events appears to justify its continued use.Basis for
Study The authors conducted a meta-analysis in an attempt
to resolve conflicting data over whether statin use increases the
risk of diabetes.
Detailed Summary of Study The authors located and
analyzed 13 randomized controlled trials of statins (n = 91,140
subjects) that tracked the development of diabetes.
Results/Body Over a mean of 4 years, statin users
had a slightly increased risk of developing diabetes (odds ratio
1.09) compared to those assigned to placebo. “The risk is low both
in absolute terms and when compared with the reduction in coronary
events. Clinical practice in patients with moderate or high
cardiovascular risk or existing cardiovascular disease should not
change.”
Sources & Other Links Sattar N, Preiss D, Murray HM,
Welsh P, Buckley BM, de Craen AJ, Seshasai SR, McMurray JJ, Freeman
DJ, Jukema JW, Macfarlane PW, Packard CJ, Stott DJ, Westendorp RG,
Shepherd J, Davis BR, Pressel SL, Marchioli R, Marfisi RM, Maggioni
AP, Tavazzi L, Tognoni G, Kjekshus J, Pedersen TR, Cook TJ, Gotto
AM, Clearfield MB, Downs JR, Nakamura H, Ohashi Y, Mizuno K, Ray KK,
Ford I.
Statins and risk of incident diabetes: a collaborative meta-analysis
of randomised statin trials. Lancet.
2010 Feb 27;375(9716):735-742.
-
2009-2010 INFLUENZA
SEASON; INFLUENZA ACTIVITY REMAINED AT APPROXIMATELY AT THE SAME
LEVELS AS WEEK
8
Synopsis:
- 174 (5.1%) specimens tested by U.S. World Health
Organization (WHO) and National Respiratory and Enteric Virus
Surveillance System (NREVSS) collaborating laboratories and
reported to CDC/Influenza Division were positive for influenza.
- All subtyped influenza A viruses reported to CDC were 2009
influenza A (H1N1) viruses.
- The proportion of deaths attributed to pneumonia and
influenza (P&I) was below the epidemic threshold.
- No influenza-associated pediatric deaths were reported.
- The proportion of outpatient visits for influenza-like
illness (ILI) was 1.9% which is below the national baseline of
2.3%. Three of 10 regions (Regions 4, 7, and 9) reported ILI at
or above region-specific baseline levels.
- No states reported widespread influenza activity, five
states reported regional influenza activity, Puerto Rico and six
states reported local influenza activity, Guam, and 33 states
reported sporadic influenza activity, the U.S. Virgin Islands
and six states reported no influenza activity, and the District
of Columbia did not report.
-
PLAVIX (CLOPIDOGREL) HAS
REDUCED EFFECTIVENESS IN PATIENTS WHO ARE POOR METABOLIZERS OF THE
DRUG
FDA notified healthcare professionals and
patients that a Boxed Warning has been added to the prescribing
information for Plavix, an anti-blood clotting medication. The Boxed
Warning in the drug label will include information to:
- Warn about reduced effectiveness
in patients who are poor metabolizers of Plavix. Poor
metabolizers do not effectively convert Plavix to its active
form in the body.
- Inform healthcare professionals that tests are available to
identify genetic differences in CYP2C19 function.
- Advise healthcare professionals to consider use of other
anti-platelet medications or alternative dosing strategies for
Plavix in patients identified as poor metabolizers.
Plavix is given to reduce the risk of Heart attack, unstable
Angina, Stroke, and cardiovascular death in patients with
Cardiovascular Disease. Plavix works by decreasing the activity of
blood cells called platelets, making platelets less likely to form
blood clots. A data summary and additional information for
healthcare professionals and patients are provided in the linked
Drug Safety Communication.
-
BLOOD TRANSFUSION FOR PREVENTING STROKE IN PEOPLE
WITH SICKLE CELL DISEASE
Authors
Hirst Ceri, Wang Winfred C
Review Group Cochrane Cystic Fibrosis and Genetic
Disorders Group
Abstract In sickle cell disease (SCD), a common
inherited haemoglobin disorder, abnormal haemoglobin distorts red
blood cells, causing anaemia, vaso-occlusion and dysfunction in most
body organs. Stroke affects around 10% of children with sickle cell
anaemia and recurrence is likely. Chronic blood transfusion dilutes
the sickled red blood cells, reducing the risk of vaso-occlusion and
stroke. However, side effects can be severe.
Objectives:
To assess risks and benefits of chronic blood transfusion
regimens in people with SCD to prevent first stroke or recurrences.
Search strategy:
We searched the Cochrane Cystic Fibrosis and Genetic Disorders
Group Trials Register, comprising references identified from
comprehensive electronic database searches and handsearches of
relevant journals and conference proceedings.Last search of the
Group's Trials Register: 22 May 2009.
Selection criteria:
Randomised and quasi-randomised controlled trials comparing blood
transfusion as prophylaxis for stroke in people with SCD to
alternative or no treatment.
Data collection and analysis:
Both authors independently assessed trial quality and extracted
data.
Main results:
Searches identified two eligible trials. One compared a chronic
transfusion regimen for maintaining sickle haemoglobin lower than
30% with standard care in 130 children with SCD judged (through
transcranial doppler ultrasonography) as high-risk for first stroke.
During the trial, 11 children in the standard care group suffered a
stroke compared to one in the transfusion group. This 92% relative
risk reduction meant the trial was terminated early. Thirty months
treatment was planned, but median follow up was 21.1 months. The
transfusion group had a high complications rate: iron overload;
alloimmunisation; and transfusion reactions. The second trial
investigated risk of stroke when transfusion was stopped after at
least 30 months. The trial closed early due to a significant
difference in risk of stroke between participants who stopped
transfusion and those who continued (for whom it was deemed unsafe
to recommend discontinuation), as measured by abnormal velocities on
Doppler examinations, OR 0.02 (95% CI 0.00 to 0.43). No trials were
identified investigating transfusion for preventing recurrence of
stroke.
Authors' conclusions:
These trials demonstrated a significantly reduced risk of stroke
in participants receiving regular blood transfusions. Data from a
follow-up trial indicate individuals may revert to former risk
status if transfusion is discontinued. Degree of risk must be
balanced against the burden of chronic transfusions. Further
research is required examining the use of transfusion in preventing
secondary stroke, and further defining risk factors for stroke, to
avoid unnecessarily starting children on blood transfusions.
Implications The STOP trial demonstrated a 90%
relative reduction in risk of first stroke in high-risk children
receiving regular blood transfusions, over a median follow up time
of 21.1 months (STOP 1998). This must be balanced against the
adverse effects and costs of a chronic transfusion regimen. The STOP
2 trial found that it is not safe to discontinue transfusion
therapy, even after 30 months of treatment, in these high risk
individuals (STOP 2 2005). No randomised controlled trials were
found regarding prevention of secondary stroke by blood transfusion
in people with sickle cell disease.
Citation Hirst C, Wang WC. Blood transfusion for
preventing stroke in people with sickle cell disease. Cochrane
Database of Systematic Reviews 2009, Issue 4. Art. No.: CD003146.
DOI: 10.1002/14651858.CD003146.
-
CURRENT USE OF ASPIRIN AND ANTITHROMBOTIC AGENTS
IN PATIENTS WITH ATHEROTHROMBOTIC DISEASE
Summary About 25% of outpatients
with vascular disease or at risk for it did not take aspirin, and
15% did not take any antithrombotic medication.Basis for Study
"Despite its proven efficacy, low cost, and wide availability,
aspirin remains underused." As part of the Reduction of
Atherothrombosis for Continued Health Registry, the authors
identified predictors of aspirin use in outpatients with
atherothrombosis.
Detailed Summary of Study Demographic information
and data on aspirin use were collected from 25,686 outpatients with
atherothrombosis or at least three risk factors for it.
Results/Body Aspirin use was more likely in men,
whites, patients age <65 and residents of the Midwest. About two
thirds of the aspirin users took low-dose aspirin. Antithrombotic
use was more common in whites, patients with atrial fibrillation or
vascular disease, patients taking" other
risk-reducing medications" and patients being treated by
cardiologists. Antithrombotic use was less likely in women, smokers
and diabetics.
Sources & Other Links
<> Cannon CP, Rhee KE, Califf RM, Boden WE, Hirsch AT, Alberts
MJ, Cable G, Shao M, Ohman EM, Steg PG, Eagle KA, Bhatt DL; REACH
Registry Investigators.
Current use of aspirin and antithrombotic agents in the United
States among outpatients with atherothrombotic disease (from the
REduction of Atherothrombosis for Continued Health [REACH]
Registry). Am J Cardiol.
2010 Feb 15;105(4):445-52
-
EVEN SLIGHT REDUCTIONS IN DIETARY SALT COULD
SUBSTANTIALLY REDUCE CARDIOVASCULAR DISEASE
Summary "Modest reductions in dietary salt could
substantially reduce cardiovascular events and medical costs and
should be a public health target."
Basis for Study The authors projected the impact
that lowering dietary salt levels would have on the incidence of
cardiovascular disease in America.
Detailed Summary of Study The incidence of coronary
heart disease, stroke, and myocardial infarction was estimated
assuming a reduction in dietary salt intake by up to 3 g per day
(1,200 mg sodium/day). The authors also examined the efficacy of
salt reduction in various groups, compared the impact with that of
other public-health efforts, and compared the cost-effectiveness of
salt reduction vs. treatment of hypertension with medications.
Results/Body "Reducing dietary salt by 3 g per day is
projected to reduce the annual number of new cases of CHD by 60,000
to 120,000, stroke by 32,000 to 66,000, and myocardial infarction by
54,000 to 99,000 and to reduce the annual number of deaths from any
cause by 44,000 to 92,000." It would save"194,000 to 392,000
quality-adjusted life-years and $10 billion to $24 billion in health
care costs annually." Benefits were seen in all the groups analyzed,
and salt reduction was found to be a more cost-effective way to
reduce blood pressure than antihypertensive medications.
"The
cardiovascular benefits of reduced salt intake are on par with the
benefits of population-wide reductions in tobacco use, obesity, and
cholesterol levels."
Sources & Other Links Bibbins-Domingo K, Chertow GM,
Coxson PG, Moran A, Lightwood JM, Pletcher MJ, Goldman L.
Projected effect of dietary salt reductions on future cardiovascular
cisease. N Engl J Med. 2010
Feb 18;362(7):590-599
-
SEVERELY OBESE TEENS LOSE MORE WEIGHT WITH
GASTRIC BANDING THAN LIFESYTLE INTERVENTION
Summary Severely obese adolescents who underwent
laparoscopic adjustable gastric banding lost significantly more
weight, reduced their risk of metabolic syndrome and improved their
quality of life compared to those who took part in a lifestyle
intervention. However, revision operations were common in the
surgical group.Basis for Study This prospective
randomized trial from Australia compared the outcomes of these two
treatments in severely obese teens.
Detailed Summary of Study Subjects age 14 to 18 with
a BMI >35 underwent gastric banding (n = 25) or took part in a
supervised lifestyle intervention (n = 25). Weight loss, metabolic
syndrome, insulin resistance, quality of life and adverse events was
noted after 2 years in 24 of the gastric banding patients and 18 of
the lifestyle intervention participants.
Results/Body "Twenty-one (84%) in the gastric banding and
3 (12%) in the lifestyle groups lost more than 50% of excess weight,
corrected for age. "Mean weight loss was 34.6 kg in the gastric
banding group and 3.0 kg in the lifestyle intervention group. 9 of
the 25 patients in the gastric banding group had metabolic syndrome
before surgery and none had it at follow-up; corresponding figures
for the lifestyle group were 10/25 at baseline and 4/18 at follow-up."The
gastric banding group experienced improved quality of life with no
perioperative adverse events. However, 8 operations (33%) were
required in 7 patients for revisional procedures either for proximal
pouch dilatation or tubing injury during follow-up."
Sources & Other Links O'Brien PE, Sawyer SM, Laurie
C, Brown WA, Skinner S, Veit F, Paul E, Burton PR, McGrice M,
Anderson M, Dixon JB.
Laparoscopic adjustable gastric banding in severely obese
adolescents: a randomized trial. JAMA.
2010 Feb 10;303(6):519-26.
-
LONGER NEEDLES SHOULD BE USED WHEN GIVING
HEPATITIS B VACCINE TO OBESE ADOLESCENTS
Summary Obese adolescents who received the hepatitis B
vaccine using a 1.5-inch needle had significantly higher antibody
titers than those immunized with a 1-inch needle.Basis for
Study The authors determined whether a shorter needle’s
inability to penetrate the deltoid fat pad in obese adolescents
could account for their lower antibody titers.
Detailed Summary of Study
<> Obese adolescents were randomized to receive the hepatitis B
vaccine using a 1-inch or a 1.5-inch needle. Antibody titers were
compared after vaccination.
Results/Body
<> Median titers were 189.8 mIU/mL with the 1-inch needle and
345.4 mIU/mL with the 1.5-inch needle."Needle length accounts for a
significant portion of the discrepancy in immune response to HBV
vaccine that is seen among those with obesity."
Sources & Other Links Middleman AB, Anding R, Tung
C.
Effect of needle length when immunizing obese adolescents with
hepatitis B vaccine. Pediatrics.
2010 Feb 8. [Epub ahead of print].
-
ORAL BISPHOSPHAONATES; ONGOING SAFETY REVIEW OF
ATYPICAL SUBTROCHANTERIC FEMUR FRACTURES
FDA notified healthcare professionals and
patients that at this point, the data that FDA has reviewed have not
shown a clear connection between bisphosphonate use and a risk of
atypical subtrochanteric femur fractures. FDA is working with
outside experts, including members of the recently convened American
Society of Bone and Mineral Research Subtrochanteric Femoral
Fracture Task Force, to gather more information and evaluate the
issue further.FDA recommends that healthcare professionals follow
the recommendations in the drug label when prescribing oral
bisphosphonates.
Patients should continue taking oral bisphosphonates unless told
by their healthcare professional to stop. Patients should talk to
their healthcare professional if they develop new hip or thigh Pain
or have any concerns with their medications.
[03/10/2010 -
Drug Safety Communication: Ongoing safety review of oral
bisphosphonates and atypical subtrochanteric femur fractures -
FDA]
-
WINRHO SDF (Rho(D) IMMUNE GLOBULIN INTRAVENOUS
(HUMAN): RISK OF INTRAVASCULAR HEMOLYSIS IN PATIENTS WITH IMMUNE
THROMBOCYTOPENIC PURPURA
Cangene, Baxter and FDA notified healthcare
professionals that cases of intravascular hemolysis (IVH) and its
complications, including fatalities, have been reported in patients
treated for immune thrombocytopenic purpura (ITP) with WinRho SDF.
IVH can lead to clinically compromising anemia and multi-system
organ failure including acute respiratory distress syndrome. Serious
complications including severe anemia, acute renal insufficiency,
renal failure and disseminated intravascular coagulation have also
been reported. Fatal outcomes associated with IVH and its
complications have occurred most frequently in patients of advanced
age (age over 65) with co-morbid conditions.The Boxed Warning
informs healthcare professionals that:
- Patients should be closely monitored in a
health care setting for at least eight hours after adminstration
- A dipstick urinalysis should be performed
at baseline, 2 hours, 4 hours after administration and prior to
the end of the monitoring.
- patients should be alerted to and monitor
for signs and symptoms of IVH, including back pain, shaking
chills, fever, ad discolored urine or hematuria. Absence
of these signs ad/or symptoms of IVH within eight hours do not
indicate IVH cannot occur subsequently
- If signs and/or symptoms of IVH are
present or if IVH is suspected after WinRho administration,
post-treatment laboratory tests should be performed including
plasma hemoglobin, urinalysis, haptoglobin, LDH and plasm
bilirubin (direct and indirect).
-
INSULIN-SENSITIZING DRUGS FOR WOMEN WITH
POLYCYSTIC OVARY SYNDROME
Authors
Tang Thomas, Lord Jonathan M, Norman Robert J, Yasmin Ephia, Balen
Adam H
Review Group Cochrane Menstrual Disorders and
Subfertility Group
Abstract Polycystic ovary syndrome (PCOS) is
characterised by anovulation, hyperandrogaenemia and insulin
resistance. Hyperinsulinaemia is associated with an increase in
cardiovascular risk and the development of diabetes mellitus. If
insulin sensitising agents such as metformin are effective in
treating features of PCOS, then they could have wider health
benefits than just treating the symptoms of the syndrome.
Objectives:
To assess the effectiveness of insulin sensitising drugs in
improving reproductive outcomes and metabolic parameters for women
with PCOS and menstrual disturbance.
Search strategy:
We searched the Cochrane Menstrual Disorders & Subfertility Group
trials register (searched September 2008), the Cochrane Central
Register of Controlled Trials (Cochrane Library, third Quarter
2008), CINAHL (searched September 2008), MEDLINE (January 1966 to
September 2008), and EMBASE (January 1985 to September 2008). All
searches were rerun 13 August 2009 17 RCTs were located and await
classification.
Selection criteria:
Randomised controlled trials which investigated the effect of
insulin sensitising drugs compared with either placebo or no
treatment, or compared with an ovulation induction agent.
Data collection and analysis:
Thirty one trials (2537 women) were included for analysis, 27 of
them using metformin and involving 2150 women.
Main results:
There is no evidence that metformin improves live birth rates
whether it is used alone (Pooled OR = 1.00, 95% CI 0.16 to 6.39) or
in combination with clomiphene (Pooled OR = 1.48, 95% CI 1.12 to
1.95). However, clinical pregnancy rates are improved for metformin
versus placebo (Pooled OR = OR 3.86, 95% C.I. 2.18 to 6.84) and for
metformin and clomiphene versus clomiphene alone (Pooled OR =1.48,
95% C.I. 1.12 to 1.95) ). In the studies that compared metformin and
clomiphene alone, there was no evidence of an improved live birth
rate (OR= 0.67, 95% CI 0.44 to 1.02) but the pooled OR resulted in
improved clinical pregnancy rate in in the clomiphene group (OR =
0.63 , 95% 0.43 to 0.92), although there was significant
heterogeneity.There is also evidence that ovulation rates are
improved with metformin in women with PCOS for metformin versus
placebo (Pooled OR 2.12, 95% CI 1.50 to 3.0) and for metformin and
clomiphene versus clomiphene alone (Pooled OR = 3.46, 95% CI 1.97 to
6.07).Metformin was also associated with a significantly higher
incidence of gastrointestinal disturbance, but no serious adverse
effects were reported.
Authors' conclusions:
In agreement with the previous review, metformin is still of
benefit in improving clinical pregnancy and ovulation rates.
However, there is no evidence that metformin improves live birth
rates whether it is used alone or in combination with clomiphene, or
when compared with clomiphene. Therefore, the use of metformin in
improving reproductive outcomes in women with PCOS appears to be
limited.
Implications In agreement with the previous review,
metformin is still of benefit in improving clinical pregnancy and
ovulation rates. However, there is no evidence that metformin
improves live births whether it is used alone or in combination with
clomiphene. In addition, metformin has limited effect on weight loss
and metabolic parameters (insulin and the lipid profiles),
especially in obese women with PCOS. Therefore, the use of metformin
in improvement of reproductive outcomes or in reducing the risk of
developing metabolic syndrome in women with PCOS appears to be
limited. Furthermore, obesity poses a significant negative impact on
the pregnancy outcomes Legro 2007. Hence, anovulatory obese women
with PCOS should be advised to undergo life-style changes before
fertility treatment (The Thessaloniki ESHRE/ASRM sponsored PCOS
consensus workshop group, 2007) ESHRE/ASRM 2008.
Citation Tang T, Lord JM, Norman RJ, Yasmin E, Balen
AH. Insulin-sensitising drugs (metformin, rosiglitazone,
pioglitazone, D-chiro-inositol) for women with polycystic ovary
syndrome, oligo amenorrhoea and subfertility. Cochrane Database of
Systematic Reviews 2009, Issue 4. Art. No.: CD003053. DOI:
10.1002/14651858.CD003053.pub3.
-
GLUCOSAMINE THERAPY FOR TREATING OSTEOARTHRITIS
Authors Towheed Tanveer, Maxwell Lara,
Anastassiades Tassos P, Shea Beverley, Houpt JB, Welch Vivian,
Hochberg Marc C, Wells George AReview Group Cochrane
Musculoskeletal Group
Abstract Osteoarthritis (OA) is a common form of arthritis
and is often associated with significant disability and impaired
quality of life. This is an update of a Cochrane review first
published in 2001 and previously updated in 2005.
Objectives:
To review randomized controlled trials (RCTs) evaluating the
effectiveness and toxicity of glucosamine in OA.
Search strategy:
We searched CENTRAL and the Cochrane Database of Systematic
Reviews (The Cochrane Library), MEDLINE, PREMEDLINE, EMBASE, AMED,
ACP Journal Club, DARE (to January 2008); contacted content experts,
and handsearched reference lists and pertinent review articles.
Selection criteria:
RCTs evaluating the effectiveness and safety of glucosamine in
OA.
Data collection and analysis:
Data abstraction was performed independently by two review
authors and investigators were contacted for missing data.
Main results:
This update includes 25 studies with 4963 patients. Analysis
restricted to studies with adequate allocation concealment failed to
show any benefit of glucosamine for pain (based on a pooled measure
of different pain scales) and WOMAC pain, function and stiffness
subscales; however, it was found to be better than placebo using the
Lequesne index (standardized mean difference (SMD) -0.54; 95%
confidence interval (CI) -0.96 to -0.12). Collectively, the 25 RCTs
favoured glucosamine with a 22% (change from baseline) improvement
in pain (SMD -0.47; 95% CI -0.72 to -0.23) and a 11% (change from
baseline) improvement in function using the Lequesne index (SMD
-0.47; 95% CI -0.82 to -0.12). However, the results were not
uniformly positive and the reasons for this remain unexplained.
WOMAC pain, function and stiffness outcomes did not reach
statistical significance.RCTs in which the Rotta preparation of
glucosamine was compared to placebo found glucosamine superior for
pain (SMD -1.11; 95% CI -1.66 to -0.57) and function (Lequesne index
SMD -0.47; 95% CI -0.82 to -0.12). Pooled results for pain (SMD
-0.05; 95% CI -0.15 to 0.05) and function using the WOMAC index (SMD
-0.01; 95% CI -0.13 to 0.10) in those RCTs using a non-Rotta
preparation of glucosamine did not reach statistical significance.
Two RCTs using the Rotta preparation showed that glucosamine was
able to slow radiological progression of OA of the knee over a
three-year period (mean difference (MD) 0.32; 95% CI 0.05 to
0.58).Glucosamine was as safe as placebo in terms of the number of
participants reporting adverse reactions (relative risk ratio 0.99;
95% CI 0.91 to 1.07).
Authors' conclusions:
Pooled results from studies using a non-Rotta preparation or
adequate allocation concealment failed to show benefit in pain and
WOMAC function while those studies evaluating the Rotta preparation
showed that glucosamine was superior to placebo in the treatment of
pain and functional impairment resulting from symptomatic OA.
Implications The previous review from 2005, with 20
studies and 2570 participants, showed that glucosamine sulphate
taken orally in amounts of 1500 mg/day produced a 28% (per cent
change from baseline) benefit in pain and an increase in function of
21% (per cent change in Lequesne Index from baseline) in
osteoarthritis, without side effects.If only the best designed
studies are included, the benefit in pain and WOMAC function is no
longer present; as shown in this update which includes 25 studies
and 4963 patients. Inclusion of five new studies reduces the overall
benefit on pain to 22% and function to 11% in the Lequesne Index.
Pooled results from studies using a non-Rotta preparation or
adequate allocation concealment failed to show benefit in pain and
WOMAC function, while those studies evaluating the Rotta preparation
showed that glucosamine was superior to placebo in the treatment of
pain and functional impairment resulting from symptomatic OA. WOMAC
outcomes of pain and function showed a superiority of glucosamine
over placebo for only the Rotta preparation of glucosamine.Some
studies suggest the Rotta preparation of glucosamine sulfate may
slow radiological progression of OA of the knee over a three-year
period. The ability of glucosamine to improve symptoms and delay
radiological progression of OA affecting other joint sites also
needs further research.Glucosamine was as safe as placebo.
Citation Towheed T, Maxwell L, Anastassiades TP,
Shea B, Houpt JB, Welch V, Hochberg MC, Wells GA. Glucosamine
therapy for treating osteoarthritis. Cochrane Database of Systematic
Reviews 2009, Issue 4. Art. No.: CD002946. DOI:
10.1002/14651858.CD002946.pub2.
- INFLUENZA VACCINE MAY NOT BE BENEFICIAL IN
PATIENTS WITH CYSTIC FIBROSIS
Authors
Dharmaraj Poonam, Smyth Rosalind L
Review Group Cochrane Cystic Fibrosis and Genetic
Disorders Group
Abstract Viral respiratory tract infections in
people with cystic fibrosis (CF) have a deteriorating effect on
their lung function and disease progression. Annual influenza
vaccination is therefore commonly recommended for people with CF.
Objectives:
To assess the effectiveness of influenza vaccination for people
with CF.
Search strategy:
We searched the Cochrane Cystic Fibrosis and Genetic Disorders
Group Trials Register which comprises of references identified from
comprehensive electronic database searches and hand searching of
relevant journals and abstract books of conference proceedings. We
also contacted the companies which market the influenza vaccines
used in the trials to obtain further information about randomized
controlled trials. Date of the most recent search of the Cystic
Fibrosis Trials Register: 05 March 2009.
Selection criteria:
All randomized and quasi-randomized trials (published or
unpublished) comparing any influenza vaccine with a placebo or with
another type of influenza vaccine.
Data collection and analysis:
Two authors independently assessed study quality and extracted
data. Additional information was obtained by contacting the
investigators when it was indicated.
Main results:
Four studies enrolling a total of 179 participants with CF (143
(80%) were children aged 1 to 16 years) were included in this
review. There was no study comparing a vaccine to a placebo or a
whole virus vaccine to a subunit or split virus vaccine. Two studies
compared an intranasal applied live vaccine to an intramuscular
inactivated vaccine and the other two studies compared a split virus
to a subunit vaccine and a virosome to a subunit vaccine (all
intramuscular). The incidence of all reported adverse events was
high depending on the type of influenza vaccine. The total adverse
event rate ranged from 48 out of 201 participants (24%) for the
intranasal live vaccine to 13 out of 30 participants (43%) for the
split virus vaccine. With the limitation of a statistical low power
there was no significant difference between the study vaccinations.
None of the events were severe. All study influenza vaccinations
generated a satisfactory serological antibody response. No study
reported other clinically important benefits.
Authors' conclusions:
There is currently no evidence from randomized studies that
influenza vaccine given to people with CF is of benefit to them.
There remains a need for a well-constructed clinical study, that
assesses the effectiveness of influenza vaccination on important
clinical outcome measures.
Implications According to some national
recommendations and the practice in many units caring for people
with CF, it is advisable to vaccinate people with CF against
influenza annually. Evidence from randomized controlled studies to
support this recommendation in people with CF is lacking and
clinicians must make judgments on the benefits and risks of this
therapy in people with CF. The cost of annual influenza vaccination
may also be considered before implementing changes to current
practice. In the UK in 2008 annual influenza vaccination cost 3.55
(excluding VAT) per patient per year (RLCH Pharmacy 2009).
Citation Dharmaraj P, Smyth RL. Vaccines for
preventing influenza in people with cystic fibrosis. Cochrane
Database of Systematic Reviews 2009, Issue 4. Art. No.: CD001753.
DOI: 10.1002/14651858.CD001753.pub2.
IN
ACUTE NECK STRAIN,
CYCLOBENZAPRINE, IBUPROFEN, OR BOTH RELIEVE PAIN EQUALLY WELL
There is little benefit to routinely using or
adding cyclobenzaprine to NSAIDs for ED patients with acute cervical
strain."Basis for Study This randomized controlled
trial compared the effectiveness of the NSAID ibuprofen, the
centrally acting muscle relaxant cyclobenzaprine (Flexeril®), or
both, in ED patients with acute neck strain.
Detailed Summary of Study Adult ED patients with
cervical strain after a motor vehicle accident or a fall were
randomized to receive ibuprofen (800 mg; n = 20), cyclobenzaprine (5
mg; n = 21) or both (n = 20) three times a day for
 7
days. Pain relief and adverse events were compared. 7
days. Pain relief and adverse events were compared.
Results/Body No significant differences were found
between the treatments in terms of pain relief or adverse events.
Sources & Other Links Khwaja SM, Minnerop M, Singer
AJ.
Comparison of ibuprofen, cyclobenzaprine or
both in patients with acute cervical strain: a randomized controlled
trial. CJEM. 2010
Jan;12(1):39-44.
- 2009-2010 INFLUENZA
SEASON ACTIVITY REMAINS AT APPROXIMATELY THE SAME LEVELS AS WEEK 6.
185 (4.4%) specimens tested by U.S. World Health
Organization (WHO) and National Respiratory and Enteric Virus
Surveillance System (NREVSS) collaborating laboratories and reported
to CDC/Influenza Division were positive for influenza.All
subtyped influenza A viruses reported to CDC were 2009 influenza A
(H1N1) viruses.
The proportion of deaths attributed to pneumonia and influenza
(P&I) was below the epidemic threshold.
Three influenza-associated pediatric deaths were reported. One
death was associated with 2009 influenza A (H1N1) virus infection
and two deaths were associated with an influenza A virus for which
the subtype was undetermined.
The proportion of outpatient visits for influenza-like illness
(ILI) was 1.8% which is below the national baseline of 2.3%. Three
of 10 regions (Regions 1, 4, and 7) reported ILI above
region-specific baseline levels.
No states reported widespread influenza activity, three states
reported regional influenza activity, Puerto Rico and eight states
reported local influenza activity, the District of Columbia, Guam,
and 35 states reported sporadic influenza activity, the U.S. Virgin
Islands and four states reported no influenza activity.
- FDA
CLEARS NEW TEST FOR OVARIAN CANCER WHICH CAN HELP
IDENTIFY POTENTIAL MALIGNANCIES AND GUIDE SURGICAL DECISIONS
The U.S. Food and Drug Administration today cleared a test that can
help detect ovarian cancer in a pelvic mass that is already known to
require surgery. The test, called OVA1, helps patients and health
care professionals decide what type of surgery should be done and by
whom.
OVA1 identifies some women who will benefit from referral to a
gynecological oncologist for their surgery, despite negative results
from other clinical and radiographic tests for ovarian cancer. If
other test results suggest cancer, referral to an oncologist is
appropriate even with a negative OVA1 result.
OVA1 should be used by primary care physicians or gynecologists as
an adjunctive test to complement, not replace, other diagnostic and
clinical procedures.
OVA1 uses a blood sample to test for levels of five proteins that
change due to ovarian cancer. The test combines the five separate
results into a single numerical score between 0 and 10 to indicate
the likelihood that the pelvic mass is benign or malignant.
OVA1 is intended only for women, 18 years and older, who are already
selected for surgery because of their pelvic mass. It is not
intended for ovarian cancer screening or for a definitive diagnosis
of ovarian cancer. Interpreting the test result requires knowledge
of whether the woman is pre- or post-menopausal.
The American College of Obstetricians and Gynecologists and the
Society of Gynecologic Oncologists published recommendations in 2002
for the role of generalist obstetrician-gynecologists in the early
detection of ovarian cancer, which included a recommendation of
patient referral to a gynecological oncologist when specific
indicators of malignancy are present.
These recommendations and later reports indicate that patients with
ovarian cancer have improved survival when the surgery is performed
by gynecologic oncologists as opposed to general gynecologists or
surgeons.
“Tests such as OVA1 personalize and improve public health by
providing patients and health care providers with more information
to support medical decisions that impact survival rates and reduce
surgical complications,” said Jeffrey Shuren, M.D., J.D., acting
director of the FDA’s Center for Devices and Radiological Health.
The FDA reviewed a study of 516 patients, including 269 evaluated by
non-gynecological oncologists, which compared OVA1 results with
biopsy results. When combined with pre-surgical information, such as
radiography and other laboratory tests, results from the OVA1 tests
identified additional patients who might benefit from oncology
referral who were not identified using pre-surgical information
alone.
OVA1 is developed by Vermillion Inc., headquartered in Fremont,
Calif., in conjunction with researchers at The Johns Hopkins
University in Baltimore.
- COLCHICINE MARKETED AS COLCRYS NOW
FDA APPROVED
FDA notified healthcare professionals of the approval of the first
single-ingredient oral colchicine product, Colcrys, for the
treatment of familial Mediterranean fever (FMF) and acute gout
flares and of two previously uncharacterized safety concerns
associated with the use of colchicine. Oral colchicine has been used
for many years as an unapproved drug with no FDA-approved
prescribing information, dosage recommendations, or drug interaction
warnings.
FDA analyzed safety data for colchicine from adverse events reported
to the Agency, the published literature, and company-sponsored
pharmacokinetic and drug interaction studies. This analysis revealed
cases of fatal colchicine toxicity reported in certain patients
taking standard therapeutic doses of colchicine and concomitant
medications that interact with colchicine, such as clarithromycin.
These reports suggest that drug interactions affecting the
gastrointestinal absorption and/or hepatic metabolism of colchicine
play a central role in the development of colchicine toxicity. Data
submitted supporting the safety and efficacy of Colcrys in acute
gout flares demonstrated that a substantially lower dose of
colchicine was as effective as the higher dose traditionally used.
Moreover, patients receiving the lower dose experienced
significantly fewer adverse events compared to the higher dose.
Based on this information, FDA has included important safety
considerations in the approved prescribing information to assure
safe use of Colcrys and is providing background information, a data
summary and recommendations in this alert.
-
UNAPPROVED USE OF
RELENZA (ZANAMIVIR) VIA NEBULIZATION/MECHANICAL VENTILATION CAN BE
ASSOCIATED WITH FATAL OUTCOME
GlaxoSmithKline (GSK) and FDA notified healthcare professionals of a
report of the death of a patient with influenza who received Relenza
(zanamivir) Inhalation Powder which was solubilized and administered
by mechanical ventilation. Relenza (zanamivir) Inhalation Powder is
not intended to be reconstituted in any liquid formulation and is
not recommended for use in any nebulizer or mechanical ventilator.
GSK is aware that Relenza Inhalation Powder is being removed from
its FDA-approved packaging and dissolved in various solutions for
the purpose of nebulizing zanamivir for inhalation by patients with
influenza who are unable to take oral medications or unable to
inhale Relenza Inhalation Powder using the Diskhaler. Relenza or
zanamivir for nebulization have not been approved by the FDA. The
safety, effectiveness, and stability of zanamivir use by
nebulization have not been established.
Relenza Inhalation Powder should only be used as directed in the
prescribing information by using the Diskhaler device provided with
the drug product. Relenza Inhalation Powder is a mixture of
zanamivir active drug substance and lactose drug carrier. This
formulation is not designed or intended to be administered by
nebulization. There is a risk that the lactose sugar in this
formulation can obstruct proper functioning of mechanical ventilator
equipment.
- LHRH
AGONISTS FOR ADJUVANT THERAPY OF EARLY BREAST
CANCER IN PREMENOPAUSAL WOMEN
Authors
Sharma Rohini, Hamilton Anne, Beith Jane
Abstract Approximately 60% of breast cancer tumours
in premenopausal women are hormone sensitive (ER+). These patients
may be suitable for hormonal treatment. The goal of hormonal therapy
is to reduce the availability of oestrogen to the cancer cell. This
can be achieved by blocking oestrogen receptors with drugs such as
tamoxifen, suppression of oestrogen synthesis by LHRH agonists, or
ovarian ablation either surgically or by radiotherapy. Chemotherapy
can also have a hormonal action by inducing amenorrhoea in
premenopausal women.
Objectives
To assess LHRH agonists as adjuvant therapy for women with early
breast cancer.
Search strategy
The specialised register of the Cochrane Breast Cancer Group was
searched on 19 December 2006. The reference lists of related reviews
were checked. A final check of the list of trials maintained by the
Early Breast Cancer Trialists' Collaborative Group was made in
January 2008.
Selection criteria
Randomised trials of LHRH agonist versus LHRH agonist and
tamoxifen, LHRH agonist versus chemotherapy, LHRH agonist versus
ovarian ablation, or LHRH agonist versus LHRH agonist and
chemotherapy, that recruited premenopausal women with early breast
cancer.
Data collection and analysis
Data were collected from trial reports. We report estimates for
the differences between treatments on recurrence free survival,
overall survival, toxicity and quality of life using data available
in the reports of each trial. Meta-analyses were not performed
because of variability in the reporting of the trials and the need
for more mature data.
Main results
We identified 14 randomised trials, involving nearly 12,000
premenopausal women with operable breast cancer, most of whom were
ER+. The LHRH agonist in most of these trials was goserelin. For
most of the treatment comparisons there are too few trials, too few
randomised patients or too little follow-up to draw reliable
estimates of the relative effects of different treatments. Four
trials (nearly 5000 women) addressed the integration of LHRH
agonists into adjuvant hormonal therapy, showing that a combination
of an LHRH agonist and tamoxifen might be better than either alone.
Insufficient data are available to inform a choice between tamoxifen
and goserelin as sole adjuvant therapy. We included twelve trials
(more than 10,000 women) of the integration of LHRH agonists into
adjuvant chemo-hormonal therapy. Four trials assessed the effects of
an LHRH agonist compared to chemotherapy and three other trials
investigated a combination of an LHRH agonist and tamoxifen versus
chemotherapy. One trial assessed the effects of adding chemotherapy
to an LHRH agonist, five trials compared a combination of an LHRH
agonist and chemotherapy versus chemotherapy alone, and three trials
compared the combination of LHRH agonist, tamoxifen and chemotherapy
versus chemotherapy alone. No trials compared an LHRH agonist
containing regimen against chemotherapy and tamoxifen. No
significant differences in recurrence free survival or overall
survival were found between LHRH agonists, with or without adjuvant
tamoxifen, and chemotherapy for premenopausal women with ER+ tumours,
but hormonal therapy had fewer distressing side effects. The trials
point to reductions in recurrence and death for premenopausal women
with ER+ tumours who take LHRH agonists, with or without tamoxifen,
along with chemotherapy.
Authors' conclusions
For premenopausal women with early breast cancer who are not
known to be ER negative, the use of an LHRH agonist, with or without
tamoxifen as adjuvant therapy is likely to lead to a reduction in
the risk of recurrence and a delay in death. The evidence is
insufficient to support the LHRH agonists over chemotherapy, or vice
versa, in regard to recurrence free survival and overall survival,
but LHRH agonists have fewer or less severe adverse effects. Further
follow-up of women in these trials is needed to provide reliable
evidence on long term outcomes. Direct randomised comparisons of
different durations of LHRH agonists (for example, two years versus
longer) and, in the presence of uncertainty, of different LHRH
agonists among ER+ or ER unknown premenopausal women are also
needed. It is also uncertain how the findings from the CMF-based
trials in this review would relate to the use of LHRH agonists with
more modern chemotherapy regimens or the comparison of LHRH agonist
containing regimens with combinations such as chemotherapy and
tamoxifen.
Implications For premenopausal women with early
breast cancer who are not known to be ER-, the use of an LHRH
agonist, with or without tamoxifen as adjuvant therapy is likely to
lead to a reduction in the risk of a recurrence and a delay in
death. If the treatment decision is a choice between the use of an
LHRH agonist and chemotherapy, this review does not provide evidence
to choose between them on the basis of recurrence free survival or
overall survival for ER+ women, but there were fewer or less severe
adverse effects among women allocated the LHRH agonist. However, for
ER- women, chemotherapy is likely to lead to a reduction in the risk
of recurrence and a delay in death compared to an LHRH agonist. The
LHRH agonist for which there is most evidence is goserelin, given as
a 3.6 mg depot subcutaneously every 28 days for a couple of years.
- IN
NEWLY DIAGNOSED CANCER PATIENTS PROGNOSIS AFFECTS INFORMATION RECALL
BETTER THAN AGE
Summary In newly
diagnosed cancer patients, prognosis is a better indicator of
information recall than age.
Basis for Study/Article This study identified
variables affecting information recall in patients newly diagnosed
with cancer.
Detailed Summary of Study The study comprised 260
cancer patients seeing an oncologist for the first time. The visits
were audiotaped, and patients were later asked to recall details
about their diagnosis, prognosis and treatment. The amount and
accuracy of their recall were checked against the recordings.
Results/Body Prognosis had a strong influence on
recall. Patients with a poorer prognosis remembered less
information, but regardless of the prognosis, patients given more
information about prognosis remembered less. Older patients
remembered less information than younger ones, but only when a large
amount of information given.
Sources & Other Links Jansen J, et al. Does age
really matter? Recall of information to newly patients with cancer.
J Clin Oncol 2008;Oct 20 [olbp]Article
Link (JCO)
- HIGH DOSES
OF VITAMIN B DON'T SLOW COGNITIVE DECLINE IN ALZHEIMER'S DISEASE
Summary This randomized controlled
trial found that high doses of vitamin B don’t slow cognitive
decline in patients with mild to moderate Alzheimer’s disease.
Basis for Study/Article This multicenter trial assessed
whether vitamin B supplements, by decreasing homocysteine levels,
could slow the progression of Alzheimer’s disease.
Detailed Summary of Study Patients with mild to
moderate Alzheimer’s disease (MMSE score 14-26) were randomized to
receive high-dose folate (5 mg/day), vitamin B6 (25 mg/day) and
vitamin B12 (1 mg/day) (n = 202) or placebo (n = 138) for 18 months.
Change from baseline was assessed using the cognitive subscale of
the Alzheimer Disease Assessment Scale.
Results/Body Patients taking the vitamins had lower
homocysteine levels than those in the placebo group, but there were
no significant differences between the groups in terms of cognitive
function. The patients taking vitamins had “a higher quantity of
adverse events involving depression.”
Sources & Other Links
Aisen PS, et al. High-dose B vitamin supplementation and cognitive
decline in Alzheimer disease: a randomized controlled trial.
JAMA. 2008 Oct 15;300(15):1774-83.
Article Link (NCBI)
- PHENYTOIN
AND FOSPHENYTOIN ALERT
FDA is investigating new preliminary data
regarding a potential increased risk of serious skin reactions
including Stevens Johnson syndrome (SJS) and toxic epidermal
necrolysis (TEN) from phenytoin therapy in Asian patients positive
for a particular human leukocyte antigen (HLA) allele, HLA-B*1502.
This allele occurs almost exclusively in patients with ancestry
across broad areas of Asia, including Han Chinese, Filipinos,
Malaysians, South Asian Indians, and Thais. Because fosphenytoin is
a prodrug and is converted to phenytoin after administration, any
concern regarding this association is also applicable to
fosphenytoin. Phenytoin and fosphenytoin are used to control tonic-clonic
(grand mal) and complex-partial seizures in epilepsy.A recent FDA
Information for Healthcare Professionals sheet (12/12/2007),
described an increased risk of SJS/TEN with another antiepileptic
drug, carbamazepine, in Asian ancestry patients with the HLA-B*1502
allele.
The FDA is working to identify additional information to evaluate
the possible risk of SJS/TEN from phenytoin and fosphenytoin in
patients with HLA-B*1502. Until the evaluation is completed,
healthcare providers who are considering the use of phenytoin or
fosphenytoin should be aware of the risks and benefits described in
the current prescribing information for this drug.
Because this new data suggests a possible association between HLA-B*1502
and phenytoin or fosphenytoin-induced SJS/TEN, and because of the
known association between phenytoin and SJS/TEN, healthcare
providers should consider avoiding phenytoin and fosphenytoin as
alternatives for carbamazepine in patients who test positive for HLA-B*1502.
- GINKGO
EVALUATION OF MEMORY (GEM) STUDY FAILS TO
SHOW BENEFIT IN PREVENTING DEMENTIA IN THE ELDERLY
In this news release written by
the National Institute on Aging, the dietary supplement Ginkgo
biloba was found to be ineffective in reducing the development of
dementia and Alzheimer's disease in older people, according to a
study published in the "Journal of the American Medical
Association. To read more, visit:
nia.nih.gov/Alzheimers/ResearchInformation/NewsReleases/PR20081119ginkgo.htm
- PSYCHOSOCIAL
AND PHARMACOLOGICAL TREATMENTS VERSUS PHARMACOLOGICAL
TREATMENTS FOR OPIOD DETOXIFICATION
Authors Amato L, Minozzi S, Davoli M, Vecchi S,
Ferri MMF, Mayet S.
Review Group Cochrane Drugs and Alcohol Group
Abstract Different pharmacological approaches aimed
at opioid detoxification are effective. Nevertheless a majority of
patients relapse to heroin use, and relapses are a substantial
problem in the rehabilitation of heroin users. Some studies have
suggested that the sorts of symptoms which are most distressing to
addicts during detoxification are psychological rather than
physiological symptoms associated with the withdrawal syndrome.
Objectives
To evaluate the effectiveness of any psychosocial plus any
pharmacological interventions versus any pharmacological alone for
opioid detoxification, in helping patients to complete the
treatment, reduce the use of substances and improve health and
social status.
Search strategy
We searched the Cochrane Drugs and Alcohol Group trials register
(27 February 2008). Cochrane Central Register of Controlled Trials
(CENTRAL) (The Cochrane Library Issue 1, 2008), PUBMED (1996 to
February 2008); EMBASE (January 1980 to February 2008); CINAHL
(January 2003-February 2008); PsycINFO (1985 to April 2003) and
reference list of articles.
Selection criteria
Randomised controlled trials which focus on any psychosocial
associated with any pharmacological intervention aimed at opioid
detoxification. People less than 18 years of age and pregnant women
were excluded.
Data collection and analysis
Three reviewers independently assessed trials quality and
extracted data.
Main results
Nine studies involving people were included. These studies
considered five different psychosocial interventions and two
substitution detoxification treatments: Methadone and Buprenorphine.
The results show promising benefit from adding any psychosocial
treatment to any substitution detoxification treatment in terms of
completion of treatment relative risk (RR) 1.68 (95% confidence
interval (CI) 1.11 to 2.55), use of opiate RR 0.82 (95% CI 0.71 to
0.93), results at follow-up RR 2.43 (95% CI 1.61 to 3.66), and
compliance RR 0.48 (95% CI 0.38 to 0.59).
Authors' conclusions
Psychosocial treatments offered in addition to pharmacological
detoxification treatments are effective in terms of completion of
treatment, use of opiate, results at follow-up and compliance.
Although a treatment, like detoxification, that exclusively
attenuates the severity of opiate withdrawal symptoms can be at best
partially effective for a chronic relapsing disorder like opiate
dependence, this type of treatment is an essential step prior to
longer-term drug-free treatment and it is desirable to develop
adjunct psychosocial approaches that might make detoxification more
effective. Limitations to this review are imposed by the
heterogeneity of the assessment of outcomes. Because of lack of
detailed information no meta analysis could be performed to analyze
the results related to several outcomes.
Implications Psychosocial treatments offered in
addition to pharmacological detoxification treatments are effective
in term of completion of treatment, use of opiate, results at
follow-up and compliance. Although a treatment, like detoxification,
that exclusively attenuates the severity of opiate withdrawal
symptoms can be at best partially effective for a chronic relapsing
disorder like opiate dependence, this form of treatment is an
essential step prior to longer-term drug-free treatment and it is
desirable to develop adjunct psychosocial approaches that might make
detoxification more effective.
Citation Amato L, Minozzi S, Davoli M, Vecchi S,
Ferri MMF, Mayet S. Psychosocial and pharmacological treatments
versus pharmacological treatments for opioid detoxification.
Cochrane Database of Systematic Reviews 2008, Issue 3. Art. No.:
CD005031. DOI: 10.1002/14651858.CD005031.pub2.
- NOVEMBER
12, 2008
Update of Safety Review Follow-up to the
October 1, 2007 - Early Communication
about the Ongoing Safety Review of Bisphosphonates
Bisphosphonates marketed as Alendronate (Fosamax, Fosamax Plus
D)
Etidronate (Didronel)
Ibandronate (Boniva)
Pamidronate (Aredia)
Risedronate (Actonel, Actonel W/Calcium)
Tiludronate (Skelid)
Zoledronic acid (Reclast, Zometa)
On October 1, 2007, FDA announced that it was reviewing
safety data that raised concerns about a potential increased
risk for atrial fibrillation in patients treated with a
bisphosphonate drug
http://www.fda.gov/cder/drug/early_comm/bisphosphonates.htm.
An article and an accompanying letter to the editor in the May
3, 2007, issue of The New England Journal of Medicine
described increased rates of serious atrial fibrillation in two
different studies of women ages 65 to 89 years old with
osteoporosis treated with the bisphosphonates, Reclast and
Fosamax. Data available to FDA at that time, including data from
the NDA approval of Reclast for osteoporosis, showed an
increased risk of serious atrial fibrillation and this risk was
reflected in the Reclast labeling. After our review, based on
the data available at this time, healthcare professionals should
not alter their prescribing patterns for bisphosphonates and
patients should not stop taking their bisphosphonate medication.
On October 1, 2007, FDA began requesting placebo-controlled
clinical trial information from the sponsors of alendronate,
ibandronate, risedronate, and zoledronic acid in order to
explore the potential risk for atrial fibrillation in male and
female patients treated with these bisphosphonate drugs.
The data submitted by the four sponsors included data on
19,687 bisphosphonate-treated patients and 18,358
placebo-treated patients who were followed for 6 months to 3
years.
The occurrence of atrial fibrillation was rare within each
study, with most studies containing 2 or fewer events. The
absolute difference in event rates between each of the
bisphosphonate and placebo arms varied from 0-3 per 1,000.
One large study of zoledronic acid showed a statistically
significant increase in the rate of serious atrial fibrillation
events. However, across all studies, no clear association
between overall bisphosphonate exposure and the rate of serious
or non-serious atrial fibrillation was observed. Increasing dose
or duration of bisphosphonate therapy was also not associated
with an increased rate of atrial fibrillation.
The FDA is aware of discordant results from the literature
and from other epidemiological studies about the incidence and
clinical course of atrial fibrillation in patients taking
bisphosphonates. FDA is exploring the feasibility of conducting
additional epidemiologic studies to examine this issue. In
addition, FDA is continuing to monitor post-market reports of
atrial fibrillation in patients who have taken bisphosphonates.
Bisphosphonates are a class of drugs used primarily to
increase bone mass and reduce the risk for fracture in patients
with osteoporosis. Bisphosphonates are also used to slow bone
turnover in patients with Paget’s disease of the bone and to
treat bone metastases and lower elevated levels of blood calcium
in patients with cancer. There are 7 FDA-approved
bisphosphonates: alendronate (Fosamax, Fosamax Plus D),
etidronate (Didronel), ibandronate (Boniva), pamidronate
(Aredia), risedronate (Actonel, Actonel W/Calcium), tiludronate
(Skelid), and zoledronic acid (Reclast, Zometa).
This follow-up communication is in keeping with FDA’s
commitment to inform the public about its ongoing safety reviews
of drugs.
The FDA urges both healthcare professionals and patients to
report side effects from the use of bisphosphonates to the FDA's
MedWatch Adverse Event Reporting program.
- CLASS
1 RECALL
VIBE Technologies, Vibrational Integrated
Bio-photonic Energizer (VIBE) Machine Multi-Frequency Field
Generator
Product:
Vibrational Integrated Bio-photonic Energizer (VIBE) Machine
Multi-Frequency Electromagnetic Field Generator
This product was manufactured and distributed from November 16,
2002 through March 19, 2008.

Use:
The company’s labeling reported that the device could be used to
treat or cure medical conditions and diseases such as:
| • |
|
cancer |
| • |
|
depression |
| • |
|
infection |
| • |
|
pain |
The firm has failed to provide FDA with any evidence to support
these claims.
Recalling Firm:
VIBE Technologies
2329 W. 10th St
Greeley, Colorado 80634-3527
Reason for Recall:
This device has not been approved by FDA, lacks safety and
effectiveness data, and is not manufactured under current good
manufacturing practices.
Public Contact:
Customers or other individuals that have been treated with this
device may contact VIBE Technologies at 1-970-356-9594.
FDA District:
Denver
FDA Comment:
On October 1, 2008, the company sent a certified letter to each
customer who purchased the device to stop using it. The letter also
included:
| • |
|
a warning label to be permanently placed on
the VIBE Machine stating that it is not a medical device and
should not be used as one. |
| • |
|
an updated operation manual/users’ guide
that contains no medical conditions or treatment claims. |
| • |
|
a certification to be signed by the user
and returned to the company acknowledging that they:
| › |
|
received the letter. |
| › |
|
attached the warning label on the
device, and |
| › |
|
understand that the VIBE Machine
does not affect the structure or function of the
human or animal body. |
|
| • |
|
a request that the user certify that they
will:
| › |
|
not promote the VIBE Machine
as a medical device. |
| › |
|
remove any medical claims from
their individual websites, and |
| › |
|
destroy any VIBE literature making
medical claims. |
|
| • |
|
a warning that failure to sign and return
the certification will result in the company refusing to
service their machine. |
Class 1 recalls are the most serious type of recall and involve
situations in which there is a reasonable probability that use of
the product will cause serious injury or death.
Health care professionals and consumers may report adverse
reactions or quality problems experienced with the use of this
product to the FDA's MedWatch Adverse Event Reporting program either
online, by regular mail or by FAX.
- FDA
ALERT
Serious Complications Associated with Transvaginal Placement of
Surgical Mesh in Repair of Pelvic Organ Prolapse and Stress Urinary
Incontinence - Issued: October 20, 2008
Dear Healthcare Practitioner:
This is to alert you to complications associated with
transvaginal placement of surgical mesh to treat Pelvic Organ
Prolapse (POP) and Stress Urinary Incontinence (SUI). Although rare,
these complications can have serious consequences. Following is
information regarding the adverse events that have been reported to
the FDA and recommendations to reduce the risks.
Nature of the Problem
Over the past three years, FDA has received over 1,000 reports
from nine surgical mesh manufacturers of complications that were
associated with surgical mesh devices used to repair POP and SUI.
These mesh devices are usually placed transvaginally utilizing tools
for minimally invasive placement.
The most frequent complications included erosion through vaginal
epithelium, infection, pain, urinary problems, and recurrence of
prolapse and/or incontinence. There were also reports of bowel,
bladder, and blood vessel perforation during insertion. In some
cases, vaginal scarring and mesh erosion led to a significant
decrease in patient quality of life due to discomfort and pain,
including dyspareunia.
Treatment of the various types of complications included
additional surgical procedures (some of them to remove the mesh), IV
therapy, blood transfusions, and drainage of hematomas or abscesses.
Specific characteristics of patients at increased risk for
complications have not been determined. Contributing factors may
include the overall health of the patient, the mesh material, the
size and shape of the mesh, the surgical technique used, concomitant
procedures undertaken (e.g. hysterectomy), and possibly estrogen
status.
Recommendations
Physicians should:
Obtain specialized training for each mesh placement technique,
and be aware of its risks.
Be vigilant for potential adverse events from the mesh,
especially erosion and infection.
Watch for complications associated with the tools used in
transvaginal placement, especially bowel, bladder and blood vessel
perforations.
Inform patients that implantation of surgical mesh is permanent,
and that some complications associated with the implanted mesh may
require additional surgery that may or may not correct the
complication.
Inform patients about the potential for serious complications and
their effect on quality of life, including pain during sexual
intercourse, scarring, and narrowing of the vaginal wall.
Additional patient information can be found on the following FDA
Consumer website at
http://www.fda.gov/cdrh/consumer/surgicalmesh-popsui.html.
- ANXIETY
PLAYS A KEY ROLE IN DEPRESSION
Summary
Anxiety plays a key role in depression, although anxiety symptoms
differ with varying levels of depression. "The relationship between
anxiety-related symptoms and depression should be considered in the
assessment of depression and evaluation of treatment strategies and
outcome."
Basis for Study/Article The authors explored the
effect that anxiety-related symptoms have in major depression.
Detailed Summary of Study Using data from four
clinical trials, the authors analyzed the relationship between
patient scores on the Hamilton Anxiety Rating Scale and the Hamilton
Depression Rating Scale.
Results/Body In general, anxiety symptoms increased
with more severe depression. Anxious mood, tension, insomnia,
concentration and memory problems and depressed mood were present at
all levels of depression, but anxiety-related somatic problems were
present only with more severe depression.
Sources & Other Links Vaccarino AL, et al. Symptoms
of anxiety in depression: assessment of item performance of the
Hamilton Anxiety Rating Scale in patients with depression.
Depress Anxiety. 2008 Sep 17.
Article Link (NCBI)
- METHYLXANTHINE
TREATMENT FOR APNEA IN PRETERM INFANT
Authors
Henderson-Smart David J, Steer Peter A
Review Group Cochrane Neonatal Group
Abstract Recurrent apnea is common in preterm
infants, particularly at very early gestational ages. These episodes
of loss of effective breathing can lead to hypoxemia and bradycardia
that may be severe enough to require resuscitation including use of
positive pressure ventilation. Methylxanthines (such as caffeine or
theophylline) have been used to stimulate breathing and prevent
apnea and its consequences.
Objectives
To determine the effects of methylxanthine treatment on the
incidence of apnea and the use of intermittent positive pressure
ventilation (IPPV), and other clinically important effects in
preterm infants with recurrent apnea.
Search strategy
Searches were made of the Cochrane Central Register of Controlled
Trials (CENTRAL, The Cochrane Library, Issue 4, 2007), the Oxford
Database of Perinatal Trials, MEDLINE (1966 to January 2008), EMBASE
(1982 - January 2008), previous reviews including cross references,
abstracts, conferences and symposia proceedings, expert informants,
journal hand searching mainly in the English language.
Selection criteria
All trials utilizing random or quasi-random patient allocation in
which methylxanthine (theophylline or caffeine) was compared with
placebo or no treatment for apnea in preterm infants were included.
Data collection and analysis
Methodological quality was assessed independently by the two
review authors. Data were extracted independently by the two review
authors. Treatment effects were expressed as relative risk (RR) and
risk difference (RD) and their 95% confidence intervals, using a
fixed effect model. For significant results, the inverse of the risk
difference (1/RD) was used to calculate the number needed to treat (NNT).
Main results
The results of five trials that enrolled a total of 192 preterm
infants with apnea indicate that methylxanthine therapy leads to a
reduction in apnea and use of IPPV in the first two to seven days.
There are insufficient data to adequately evaluate side effects and
no data to examine effects within different gestational age groups.
There are no data in the included studies that examine long-term
effects.
Authors' conclusions
Methylxanthines are effective in reducing the number of apneic
attacks and the use of mechanical ventilation in the two to seven
days after starting treatment. In view of its lower toxicity,
caffeine would be the preferred drug. The effects of methylxanthines
on long-term outcomes will be addressed in data from the trial
awaiting assessment (CAP Trial 2006).
Implications Methylxanthines are effective in
reducing the number of apneic attacks in the short-term and in
reducing the use of mechanical ventilation. In view of its lower
toxicity, caffeine would be the preferred drug. In included studies,
the safety of methylxanthine therapy is uncertain, especially in
terms of lack of long-term growth and neurodevelopment outcomes.
Citation Henderson-Smart DJ, Steer PA.
Methylxanthine treatment for apnea in preterm infants. Cochrane
Database of Systematic Reviews 2008, Issue 3. Art. No.: CD000140.
DOI: 10.1002/14651858.CD000140.
- ARIPIPRAZOLE
VERSUS TYPICAL ANTIPSYCHOTIC DRUGS FOR SCHIZOPHRENIA
Authors Bhattacharjee Jayanti, El-Sayeh Hany George G
Review Group Cochrane Schizophrenia Group
Abstract Aripiprazole is a relatively new
antipsychotic drug, said to be the prototype of a new third
generation of antipsychotics; the so-called dopamine-serotonin
system stabilisers. In this review we examine how the efficacy and
tolerability of aripiprazole differs from that of typical
antipsychotics.
Objectives
To evaluate the effects of aripiprazole compared with other
typical antipsychotics for people with schizophrenia and
schizophrenia-like psychoses.
Search strategy
We searched the Cochrane Schizophrenia Group Trials Register
(November 2007) which is based on regular searches of BIOSIS,
CENTRAL, CINAHL, EMBASE, MEDLINE and PsycINFO. We inspected
references of all identified studies for further trials. We
contacted relevant pharmaceutical companies, drug approval agencies
and authors of trials for additional information.
Selection criteria
We included all randomised trials comparing aripiprazole with
typical antipsychotics in people with schizophrenia or
schizophrenia-like psychosis.
Data collection and analysis
We extracted data independently. For dichotomous data we
calculated relative risks (RR) and their 95% confidence intervals
(CI) on an intention-to-treat basis, based on a random effects
model. We calculated numbers needed to treat/harm (NNT/NNH) where
appropriate. For continuous data, we calculated weighted mean
differences (WMD) again based on a random effects model. We have
contacted representatives of Bristol Myers Squibb pharmaceuticals
(UK) for additional data.
Main results
We included nine randomised trials involving 3122 people
comparing aripiprazole with typical antipsychotic drugs. None of the
studies reported on relapse - our primary outcome of interest.
Attrition from studies was high and data reporting poor.
Participants given aripiprazole were comparable to those receiving
typical drugs in improving global state and mental state.
Aripiprazole provided a significant advantage over typical
antipsychotics in terms of fewer occurrences of extra-pyramidal
symptom (n=968, 3 RCT, RR 0.46 CI 0.3 to 0.9, NNT 13 CI 17 to 10),
and particularly akathisia (n=897, 3 RCT, RR 0.39 CI 0.3 to 0.6, NNT
11 CI 14 to 9). Fewer participants given aripiprazole developed
hyperprolactinaemia (n=300, 1 RCT, RR 0.07 CI 0.03 to 0.2, NNT 2 CI
3 to 1). Aripiprazole presented a lesser risk of sinus tachycardia
(n=289, 1 RCT, RR 0.09 CI 0.01 to 0.8, NNT 22 CI 63 to 13) and
blurred vision (n=308, 1 RCT, RR 0.19 CI 0.1 to 0.7, NNT 14 CI 25 to
10); but enhanced risk of occurrence of dizziness (n=957, 3 RCT, RR
1.88 CI 1.1 to 3.2, NNH 20 CI 33 to 14) and nausea (n=957, 3 RCT, RR
3.03 CI 1.5 to 6.1, NNH 17 CI 25 to 13). Attrition rates were high
in both groups, although significantly more participants in the
aripiprazole group completed the study in the long term (n=1294, 1
RCT, RR 0.81 CI 0.8 to 0.9 NNT 8 CI 5 to 14).
Authors' conclusions
Aripiprazole differs little from typical antipsychotic drugs with
respect to efficacy, however it presents significant advantages in
terms of tolerability. Clearly reported pragmatic short, medium and
long term randomised controlled trials are required to replicate and
validate these findings and determine the position of aripiprazole
in everyday clinical practice.
Implications
| 1. |
|
For people with schizophrenia
Aripiprazole is not clearly more or less effective than
typical antipsychotics in terms of improving global outcomes
or mental state. However it confers a significant advantage
over older drugs in terms of fewer occurrences of
extra-pyramidal symptom related adverse events, but it is
more likely to cause dizziness and nausea.
Hyperprolactinaemia and associated complications of
unpleasant breast pain and secretion and osteoporosis do not
seem to be a significant concern with aripiprazole; while
they remain adverse effects commonly seen with the older
drugs. There appears to be a lesser chance of developing
sinus tachycardia whilst taking aripiprazole even though it
does not present any significant advantages over the typical
drugs in causing QTc abnormalities. |
| 2. |
|
For clinicians
Aripiprazole appears to be as efficacious and effective as
the comparator typical antipsychotic drugs in the included
studies. It presents a significantly favourable adverse
effect profile when compared to the older drugs. This
suggests a significant advantage over typical drugs in
ensuring compliance. However aripiprazole has been compared
to haloperidol, perphenazine, and chlorpromazine in the
studies included in this review and a sensitivity analysis
could not be conducted due to lack of adequate relevant
data; it cannot therefore be definitively concluded that it
is as effective as or better tolerated than all typical
antipsychotic drugs at various dose ranges. More studies are
needed to replicate and validate these findings. |
| 3. |
|
For managers/policy makers
No data has emerged about service outcomes. Data about
economic outcomes are minimal and insignificant. Even though
aripiprazole appears to be an efficacious and effective drug
there is inadequate data about medium and long-term
outcomes. In the context of finite resources, the lack of
good quality data leaves managers and policy makers with
difficult decisions to make. |
Citation Bhattacharjee J, El-Sayeh HGG. Aripiprazole
versus typical antipsychotic drugs for schizophrenia. Cochrane
Database of Systematic Reviews 2008, Issue 3. Art. No.: CD006617.
DOI: 10.1002/14651858.CD006617.pub3.
- WHICH
SHORT-CHAIN CARBS ARE THE VILLAINS IN IBS?
Researchers challenged IBS patients with dietary fructose,
fructans, and glucose.
Malabsorption of fructose and other short-chain carbohydrates is
thought to produce symptoms of irritable bowel syndrome (IBS).
Common dietary sources of fructose include fruits, honey, and
high-fructose corn syrup. Some carbohydrates, such as fructo-oligosaccharides
(fructans) and galactosaccharides (e.g., raffinose), cannot be
absorbed by humans.
Now, in a double-blind, randomized, crossover trial, researchers
have assessed the effects of fructose and fructans (alone or in
combination) as dietary triggers of IBS symptoms. Twenty-five
patients with known fructose malabsorption were challenged by
graded-dose introduction of fructose, fructans, the combination, or
a glucose control administered as drinks with meals for a 2-week
test period, followed by a 10-day washout period.
In a dose-dependent manner, fructose reproduced IBS symptoms in 70%
of patients, fructans reproduced symptoms in 77%, and the
combination induced symptoms in 79%. Only 14% of those challenged
with glucose showed IBS symptoms (P≤0.002).
Comment: Up to 40% of patients with IBS have been
shown to absorb fructose incompletely (JW Gastroenterol Sep 28
2007). In this study, IBS symptoms were induced by either fructose
or fructans, indicating that symptoms are reproduced by the bowel’s
response to delivery of undigested carbohydrates to the colon and
distal small bowel. These data supply more evidence to suggest that
carbohydrate malabsorption plays a role in the pathogenesis of IBS
symptoms.  Douglas K. Rex, MD
Douglas K. Rex, MD
- NICONTINIC
ACID – THE NEW OLD WONDER DRUG
Many patients with coronary heart disease (CHD)
or its equivalent will need a >50% reduction in low-density
lipoprotein (LDL) cholesterol to achieve the LDL goal of <100 mg/dl.
There are also patients with what the National Cholesterol Education
Program calls “atherogenic dyslipidemia,” which includes a nasty
metabolic stew of elevated triglycerides, low high-density
lipoprotein (HDL) cholesterol, prothrombotic and proinflammatory
states, and a preponderance of small, dense LDL particles, which are
highly atherogenic and strongly predict cardiovascular events
(Slide1)1
Moreover, all of the processes involved in atherogenesis can be
exacerbated by insulin resistance and/or the metabolic syndrome
(Slide 2).2
There are numerous treatments that, to varying degrees, affect
atherogenic dyslipidemia
(Slide 3). While statins have dramatic effects on LDL
cholesterol, they have little impact on the overall atherogenic
lipoprotein profile (ALP). Interventions that improve ALP include
fat weight loss, exercise, and good control of diabetes. One therapy
that is particularly effective at improving ALP is nicotinic acid.2
(When the biological significance of nicotinic acid was recognized,
there was a desire to distinguish it from nicotine; thus, it was
named niacin from the words “nicotinic acid vitamin.”)
In recent years, niacin has gained recognition as an
atheroprotective agent, in part because of its capacity to lower
plasma levels of cholesterol, triglycerides, and very-low- and
low-density lipoproteins. Also, of currently approved drugs, niacin
is the most effective at raising HDL cholesterol levels. However,
there have been concerns, too, that niacin might increase insulin
resistance and have adverse effects on blood glucose levels.
Combination Therapy
Current guidelines recommend consideration of combination drug
therapy to achieve optimal low-density LDL cholesterol lowering and
broader lipid-altering effects when treating hypercholesterolemic
patients at high risk for atherosclerotic cardiovascular events.1
Because statins and niacin have potentially complementary actions,
several studies have evaluated combination regimens.
For example, investigators sought to determine whether intensive
lipid therapy with a niacin-containing regimen would have a
beneficial effect on cardiovascular disease, despite any increase in
plasma glucose and insulin resistance in subjects with the metabolic
syndrome. They evaluated 3 years of treatment with slow-release
niacin plus simvastatin (N+S) on both angiographic and clinical
outcomes in 160 subjects with coronary artery disease (CAD) and low
levels of HDL from the HDL-Atherosclerosis Treatment Study (HATS).3
Treating atherogenic dyslipidemia with combination therapy led to
substantial benefits in terms of stenosis progression and clinical
events, independently of whether the patient had metabolic syndrome
or was insulin resistant. During the 3-year period, the beneficial
effect of niacin in combination with simvastatin appeared to offset
a modest adverse effect of niacin on glucose metabolism and insulin
resistance in higher risk patients, “as long as careful attention is
paid to glycemic control.”
In another study, niacin extended release (niacin-ER) plus
lovastatin was comparable to atorvastatin 10 mg and more effective
than simvastatin 20 mg in reducing LDL cholesterol.4
The combination also was more effective in increasing HDL
cholesterol than either atorvastatin or simvastatin and provided
greater global improvements in non-HDL cholesterol, triglycerides,
and lipoprotein(a)
(Slide 4).
Recently, investigators evaluated ezetimibe/simvastatin (E/S) plus
niacin-ER in patients with type IIa or IIb hyperlipidemia.5
In this 24-week multicenter, double-blind study, 1,220 patients were
randomized to treatment with E/S (10/20 mg/day), the same range of
E/S per day plus niacin (titrated to 2 g/day), or niacin alone
(titrated to 2 g/day).
Coadministration of E/S with niacin-ER resulted in numerous
beneficial effects
(Slide 5), including significantly greater reductions in LDL
cholesterol, non-HDL cholesterol, triglycerides, apolipoprotein B,
and lipid/lipoprotein ratios, compared with either agent alone (p <
0.001). The combination increased levels of apolipoprotein A-I and
HDL cholesterol significantly more than E/S (p < 0.001), and reduced
high-sensitivity C-reactive protein levels significantly more than
niacin alone (p = 0.005). The three-drug regimen was generally well
tolerated aside from some niacin-associated flushing.
Safety of Combo Rx
In a recent State-of-the-Art paper for JACC, Davidson and
Robinson reviewed the safety of aggressive lipid management.6
In a pooled analysis, ezetimibe + simvastatin 80 mg on average
resulted in a 57% reduction in LDL, and ezetimibe + atorvastatin 80
mg in 60% reduction in LDL.7
E/S resulted in a similar rate of treatment-related discontinuation
as simvastatin monotherapy. No differences in muscle-related adverse
events were found between 4,558 subjects receiving E/S and 2,563
subjects who received simvastatin alone in this analysis of 17
12-week trials. Hepatic enzyme elevations ≥3x ULN on two or more
occasions occurred in 1.4% of 925 ezetimibe + statin-treated
subjects compared with 0.4% of 936 statin-only subjects. However,
hospitalization for hepatic events was no higher for ezetimibe +
statin combinations than for statin monotherapy.
How does the addition of niacin to a statin effect safety endpoints?
As mentioned, HATS randomized 160 subjects to placebo or to
simvastatin + niacin (mean doses of simvastatin 13 mg and niacin 2.4
g). No cases of persistent ALT or CK elevations were found, and no
cases of myopathy or rhabdomyolysis were reported. The ongoing
AIM-HIGH trial will evaluate whether the addition of niacin-ER to
simvastatin will result in a cardiovascular risk reduction greater
than expected based on the degree of LDL lowering.
Safety data also were recently published from both the OCEANS and
SEACOAST studies evaluating niacin-ER and simvastatin.8,9
Combination therapy was consistent with the safety profile of each
individual component.
In April 2008, investigators published the results of adverse events
reported to the U.S. Food and Drug Administration (FDA).10
The analyses demonstrated that niacin-ER has a significantly better
safety profile compared with other niacin formulations and compares
favorably with other commonly used lipid-altering drugs, including
statins and fibrates. In addition, analyses of FDA adverse event
reports of the pill combining lovastatin and niacin-ER suggest that
the safety of combination therapy to comparable with the safety of
each of the drugs alone.
At about the same time, Goldberg and Jacobson reported the results
of an extensive literature review evaluating the effects of niacin
on glucose control in patients with dyslipidemia.11
They found that niacin (≤2.5 g/d), alone or in combination with
statins, has only modest, transient or reversible effects on plasma
glucose, and these effects are “typically amenable to adjustments in
oral hypoglycemic regimens without discontinuing niacin.”
What about triple-drug combination therapy? In the previously
mentioned study of E/S with or without niacin therapy, triple
therapy was generally well tolerated and showed a safety profile
consistent with prior experience using these agents alone or in
combination. This suggests that E/S plus niacin-ER may be an option
in patients at high risk for CHD including those with diabetes,
metabolic syndrome, and obesity, in whom polypharmacy otherwise
might be a concern. The rates of serious adverse events were
comparable for all treatment arms, and there were no statistically
significant differences in muscle, liver, and gastrointestinal
adverse events.
Also, the Davidson and Robinson paper cited one study that formally
evaluated the safety of triple therapy. A moderate dose of
lovastatin (40 mg) was combined with niacin 200 mg and colestipol 20
g and evaluated in a crossover trial in 29 middle-aged men with CHD.
This regimen resulted in 54-60% reduction in LDL, depending on the
niacin formulation. Only 21% of subjects reported the regimen was
"very easy" to take, although 79% thought it was "fairly easy." The
primary adverse effects were cutaneous, which were less when
sustained-release niacin formulations were used. No data on
laboratory abnormalities or musculoskeletal complaints were
reported.
This interview features H. Robert Superko, MD, FACC, renowned for
his work in metabolic heart disease diagnosis and treatment as well
as research and publications on the effects of lipoprotein
subclasses. He discusses the mechanism of action of nicotinic acid,
new formulations that are increasing the interest in niacin therapy,
and the value of using nicotinic acid in combination therapy.
Source
Content provided by the American College of Cardiology Foundation
[Cardiosource CME link for American College of Cardiology members]
- TO
MAINTAIN WEIGHT LOSS, EXERCISE EVEN MORE
Women who maintained a 10% weight loss during a 2-year study had
better eating habits and more leisure-time physical activity than
did those who regained weight lost during the first 6 months.
Experts generally recommend a minimum of 30 minutes of
moderate-intensity activity on most days of the week (150 minutes
weekly), but substantially more exercise probably is necessary to
lose weight and to keep it off. Investigators randomized 191
overweight and obese women who were attending a weight-loss clinic
into four groups: high or moderate energy expenditure (2000 vs. 1000
kcal/week) in the form of vigorous- or moderate-intensity exercise.
Participants also were instructed to maintain a prescribed,
reduced-caloric intake; all received intensive weight-loss
counseling, regular group visits, and periodic telephone contact.
Previous data from this study showed that average 12-month weight
losses of 10% and 8% from baseline were associated with high and
moderate amounts of exercise, respectively (JW Womens Health Nov 18
2003).
At 24 months, each group had regained on average about half the
weight lost during the first 6 months. However, the 47 women who
maintained weight loss of ≥10% had increased their leisure-time
physical activity from baseline by a mean of 1515 kcal weekly —
substantially more than did women whose weight returned to or
exceeded baseline (mean of 480 kcal weekly). No group maintained all
of the eating behavior improvements seen at 6 months; however, at 24
months, women who kept their weight at least 10% below baseline
retained more of the recommended eating behaviors than did other
participants.
Comment: Once again, a study illustrates the
difficulty of losing weight and keeping it off — even among highly
motivated women enrolled in a weight-loss clinic and given
significant support and resources (each participant received a
treadmill). As backsliding occurred, the women regained weight.
Those who sustained 10% weight losses during 2 years engaged in a
level of physical activity that was approximately twice the typical
public health recommendation. Considering the difficulty that
overweight adults have in maintaining substantial weight loss,
healthcare providers should continue to take a proactive stance
toward minimizing weight gain in children and young adults, while
also promoting more physical activity for all.
 Wendy
S. Biggs, MD Wendy
S. Biggs, MD
- PERSONALIZED
MEDICINE FOR QUITTING SMOKING
Another step toward personalized medicine
Assessing polymorphisms of cytochrome P450 (CYP) enzymes that
metabolize bupropion might help to predict efficacy for smoking
cessation (JW Psychiatry Nov 19 2007), but the cost-benefit ratio of
testing has not seemed dramatic. Because people who metabolize
nicotine rapidly have low between-cigarette nicotine levels and poor
success in quitting smoking with nonpharmacologic treatments, these
researchers investigated whether a marker of nicotine metabolism
rate (NMR) would predict quit rates. In a 10-week study, 414 smokers
(average, 1 pack/day) were randomized to counseling plus bupropion
or placebo. NMR was measured by the ratio of trans-3´-hydroxycotinine
to cotinine, two sequential metabolites of nicotine via CYP2A6.
Among the slowest nicotine metabolizers (bottom NMR quartile),
bupropion and placebo recipients had the same rate of smoking
abstinence (32%) at the end of the trial and similar rates of
maintenance of abstinence at 6-month follow-up. In contrast, among
the fastest nicotine metabolizers (top NMR quartile), bupropion was
associated with significantly higher rates than placebo for quitting
at the end of treatment (34% vs. 10%; odds ratio, 4.84) and for
maintenance at 6 months (27% vs. 8%; OR, 4.48).
Comment: People who slowly metabolize nicotine seem
to have no need for bupropion; they get good results with behavioral
methods alone. Rapid metabolizers have poorer results and higher
relapse rates with counseling alone, presumably because their
nicotine levels drop swiftly, leading to intense craving. Nicotine
supplements also might not be helpful because they will be
eliminated too rapidly.
Nicotine metabolism, but not bupropion metabolism, is dependent on
CYP3A4; genotyping of this enzyme would predict outcomes only weakly
because various environmental factors and unidentified alleles
influence the enzyme’s activity. Measuring metabolism of both
bupropion and nicotine might be useful in predicting responders to
bupropion.
Steven Dubovsky, MD
- RANDOMIZED
COMPARISON OF GUAIAC-BASED VS. IMMUNOCHEMICAL FOBT
Douglas
K. Rex, MD
Immunochemical FOBT’s better sensitivity but lower specificity
for detecting cancer and advanced adenomas (compared with guaiac-based
FOBT) led to similar positive predictive values for the two test
types.
The Joint Colorectal Cancer Screening Guideline recommends that
fecal occult blood testing (FOBT) be performed using immunochemical
methods rather than guaiac-based methods (JW Gastroenterol Apr 4
2008). However, direct comparisons between the two test types have
been performed only in patients at high risk for, or previously
diagnosed with, colorectal cancer (CRC).
Now, investigators have prospectively compared the performance of
guaiac-based FOBT (Hemoccult II) and immunochemical FOBT (OC-Sensor)
in a general screening population. A random sample of 20,623 older
Dutch adults (age range, 50-75) underwent CRC screening with one of
the two types of tests. A standard cutoff of 100 ng/mL was used for
immunochemical FOBT. Positive results on either type of FOBT were
verified with colonoscopy.
The proportion of completed tests was significantly higher for
immunochemical FOBT than for guaiac-based FOBT (6157 vs. 4836). A
total of 456 individuals had positive FOBT results; the positivity
rate was higher with immunochemical FOBT than with guaiac-based FOBT
(5.5% vs. 2.4%; P<0.01). Immunochemical FOBT detected
cancer and advanced adenomas more often than did guaiac-based FOBT
(24 vs. 11 cases and 121 vs. 46 cases, respectively). However,
immunochemical FOBT was 2.3% less specific than was guaiac-based
FOBT for detecting cancer and 1.3% less specific for detecting
advanced adenomas.
Comment: Immunochemical FOBT’s better sensitivity
but lower specificity for detecting cancer and advanced adenomas
(compared with guaiac-based FOBT) led to similar positive predictive
values for the two test types. Although wider use of immunochemical
FOBT would result in more colonoscopies, it would also lead to the
detection of substantially more neoplasias, and the positive
predictive value would be comparable to that seen with guaiac-based
FOBT. The study’s authors could not explain the higher number of
completed immunochemical tests, but this finding indicates a strong
patient preference for immunochemical FOBT. Overall, these results
support the Joint Colorectal Cancer Screening Guideline
recommendations to abandon older guaiac-based cards in favor of
immunochemical FOBT.
- OTC COUGH
AND COLD MEDICINES - PRODUCT LABELS BEING MODIFIED TO STATE "DO NOT
USE" IN CHILDREN UNDER 4 YEARS OF AGE
10/09/2008
FDA notified healthcare professionals and consumers that the
Consumer Healthcare Products Association (CHPA) is voluntarily
modifying the product labels for consumers of over the counter (OTC)
cough and cold medicines to state "do not use" in children under 4
years of age. FDA supports CHPA members to help prevent and reduce
misuse and to better inform consumers about the safe and effective
use of these products for children. FDA continues to assess the
safety and efficacy of these products and to revise its OTC list of
approved ingredients and amounts for these medicines. Parents and
care givers should adhere to the dosage instructions and warnings on
the label that accompanies OTC cough and cold medications before
giving the product to children, and should consult their healthcare
professionals if they have any questions or concerns.
GALLBALDDER
DISEASE AND USE OF TRANSDERMAL VERSUS ORAL HORMONE REPLACEMENT
THERAPY IN POSTMENOPAUSAL WOMEN: PROSPECTIVE COHORT STUDY
Bette Liu, clinical epidemiologist1,
Valerie Beral, professor of epidemiology1,
Angela Balkwill, statistical programmer1,
Jane Green, clinical research scientist1,
Siân Sweetland, statisticial epidemiologist1,
Gillian Reeves, statistical epidemiologist1,
for the Million Women Study Collaborators
1
Epidemiology Unit, University of Oxford, Oxford OX3 7LF
Correspondence to: B Liu
Bette.Liu@ceu.ox.ac.uk
Objective To determine whether transdermal compared
with oral use of hormone replacement therapy reduces the risk of
gallbladder disease in postmenopausal women.
Design Prospective cohort study (Million Women
Study).
Setting Women registered with the National Health
Service (NHS) in England and Scotland.
Participants 1 001 391 postmenopausal women (mean
age 56) recruited between 1996 and 2001 from NHS breast screening
centers and followed by record linkage to routinely collected NHS
hospital admission data for gallbladder disease.
Main outcome measures Adjusted relative risk and
standardized incidence rates of hospital admission for gallbladder
disease or cholecystectomy according to use of hormone replacement
therapy.
Results During follow-up 19 889 women were admitted
for gallbladder disease; 17 190 (86%) had a cholecystectomy.
Compared with never users of hormone replacement therapy, current
users were more likely to be admitted for gallbladder disease
(relative risk 1.64, 95% confidence interval 1.58 to 1.69) but risks
were substantially lower with transdermal therapy than with oral
therapy (relative risk 1.17, 1.10 to 1.24 v 1.74, 1.68 to
1.80; heterogeneity P<0.001). Among women using oral therapy, equine
oestrogens were associated with a slightly greater risk of
gallbladder disease than estradiol (relative risk 1.79, 1.72 to 1.87
v 1.62, 1.54 to 1.70; heterogeneity P<0.001) and higher
doses of estrogen increased the risk more than lower doses: for
equine estrogens >0.625 mg, 1.91 (1.78 to 2.04) v ≤0.625
mg, 1.76 (1.68 to 1.84); heterogeneity P=0.02; estradiol >1 mg, 1.68
(1.59 to 1.77) v ≤1 mg, 1.44 (1.31 to 1.59); heterogeneity
P=0.003. The risk of gallbladder disease decreased with time since
stopping therapy (trend P=0.004). Results were similar taking
cholecystectomy as the outcome. Standardized hospital admission
rates per 100 women over five years for cholecystectomy were 1.1 in
never users, 1.3 with transdermal therapy, and 2.0 with oral
therapy.
Conclusion Gallbladder disease is common in
postmenopausal women and use of hormone replacement therapy
increases the risk. Use of transdermal therapy rather than oral
therapy over a five year period could avoid one cholecystectomy in
every 140 users.
- CONTINUOUS
GLUCOSE MONITORING IN TYPE 1 DIABETES
Allan S. Brett, MD
Published in Journal Watch General Medicine September
30, 2008
Continuous monitoring helped lower
HbA1c
levels in patients who were older than 24, but not in children,
adolescents, or younger adults.
Continuous glucose monitoring devices, which measure interstitial
glucose via subcutaneous sensors, now are available commercially. To
determine the value of such devices, 322 adults and children with
type 1 diabetes (glycosylated hemoglobin [HbA1c]
level, 7%–10%) were randomized to continuous glucose monitoring or
to conventional monitoring (fingerstick testing ≥4 times daily).
Three prespecified age subgroups were enrolled: 8 to 14 years, 15 to
24 years, and 25 or older. Patients used either insulin pumps or
multiple daily insulin injections and were instructed on adjusting
insulin doses according to monitoring results.
Among patients who were 25 or older, mean HbA1c
concentration decreased by a mean of 0.5 percentage points at 26
weeks in the continuous monitoring group but remained unchanged in
the conventional monitoring group — a significant difference. In
contrast, among younger patients, continuous monitoring did not
lower mean HbA1c
levels more than conventional monitoring did. Continuous monitoring
improved most secondary endpoints in the oldest patients and some
endpoints (e.g., proportion of subjects with HbA
levels <7% at 26 weeks) in the youngest patients, but among
15- to 24-year-olds, no significant differences emerged. Within the
continuous monitoring groups, those in the 15- to 24-year-old group
were less adherent to sensor use than were older or younger
patients. Rates of hypoglycemia were similar with continuous and
conventional monitoring in all age groups.
Comment: Not surprisingly, continuous glucose
monitoring was most effective in patients who were 25 or older and
was no better than conventional monitoring in adolescents and very
young adults. Continuous monitoring is expensive, has some accuracy
limitations, and requires patient motivation. Although this method
is appealing theoretically, the extent to which it will improve
long-term clinical outcomes remains to be determined.
- DECONGENSTANTS
AND ANTIHISTAMINES FOR ACUTE OTITIS MEDIA IN CHILDREN
Authors Coleman Cassie, Moore Michael
Review Group Cochrane Acute Respiratory Infections
Group
Abstract Acute otitis media (AOM) is a common and
important source of morbidity in children, although the majority of
cases resolve spontaneously. While frequently recommended,
decongestant and antihistamine therapy is of unclear benefit.
Objectives To determine the efficacy of decongestant and
antihistamine therapy in children with AOM on outcomes of AOM
resolution, symptom resolution, medication side effects, and
complications of AOM.Search strategy In this updated review, we
searched the Cochrane Central Register of Controlled Trials
(CENTRAL) (The Cochrane Library 2007, Issue 2); MEDLINE (January
2004 to May 2007); and EMBASE (July 2003 to May 2007).Selection
criteria Randomized controlled trials (RCTs) evaluating decongestant
or antihistamine treatment for children with AOM were included.
Patient-oriented outcomes were considered most relevant.
Data collection and analysis: The review authors
independently evaluated studies for inclusion, performed validity
assessments and completed data extraction. Dichotomous data were
pooled to generate relative risks; homogeneity was assessed using
approximate chi-square tests. Main results
No new studies were included following this updated search. Fifteen
trials involving 2695 people were included. Only the combined
decongestant-antihistamine group demonstrated statistically lower
rates of persistent AOM at the two week period (fixed relative risk
(RR) 0.76; 95% confidence interval (CI) 0.60 to 0.96; number needed
to treat (NNT) 10). No benefit was found for early cure rates,
symptom resolution, prevention of surgery or other complications.
There was a five to eight -fold increased risk of side effects for
those receiving an intervention, which reached statistical
significance for all decongestant groupings. Validity sub analyses
demonstrated that lower quality studies found benefit, while
analysis of those studies with higher validity scores found no
benefit of treatment. Authors' conclusions
Given lack of benefit and increased risk of side effects, these data
do not support the use of decongestant treatment in children with
AOM. There was a small statistical benefit from combination
medication use but the clinical significance is minimal and study
design may be biasing the results. Thus, the routine use of
antihistamines for treating AOM in children cannot be recommended.
Implications This review did not find sufficient
statistical or clinical benefit to decongestant, antihistamine or
combination therapy for AOM. Treatment groups, however, experienced
an increased risk of side effects. The current evidence suggests
that decongestants and/or antihistamines not be routinely used to
treat children with AOM.
Citation Coleman C, Moore M. Decongestants and
antihistamines for acute otitis media in children. Cochrane Database
of Systematic Reviews 2008, Issue 3. Art. No.: CD001727. DOI:
10.1002/14651858.CD001727.pub4.
- RECOMMENDATIONS
FOR TREATING LOW BONE DENSITY/OSTEOPOROSIS TO PREVENT FRACTURES
Summary The American
College of Physicians has made four recommendations for treating low
bone density/osteoporosis in an attempt to prevent fractures: 1)
Patients with osteoporosis and those who have had fragility
fractures should receive pharmacologic treatment; 2) Clinicians
should consider pharmacologic treatment of patients at risk for
developing osteoporosis; 3) Pharmacologic treatment should be based
on a risk/benefit assessment in individual patients; 4) More
research in needed to evaluate treatments for osteoporosis.
Basis for Study/Article The American College of
Physicians “developed this guideline to present the available
evidence on various pharmacologic treatments to prevent fracture in
men and women with low bone density or osteoporosis.”
Detailed Summary of Study The authors conducted a
literature search for relevant articles and analyzed the data.
Results/Body 1) Patients with osteoporosis and those
who have had fragility fractures should receive pharmacologic
treatment (strong recommendation, high-quality evidence); 2)
Clinicians should consider pharmacologic treatment of patients at
risk for developing osteoporosis (weak recommendation,
moderate-quality evidence); 3) Pharmacologic treatment should be
based on a risk/benefit assessment in individual patients (strong
recommendation, moderate-quality evidence); 4) More research in
needed to evaluate treatments for osteoporosis.
Sources & Other Links Qaseem A, et al. Pharmacologic
treatment of low bone density or osteoporosis to prevent fractures:
a clinical practice guideline from the American College of
Physicians. Ann Intern Med. 2008
Sep 16;149(6):404-15.
Article Link (NCBI)
- FEMORAL
NECK STRENGTH IS HIGHER IN BOYS; INTENSITY OF ACTIVITY PREDICTS
STRENGTH
Summary In 9-year-olds, the
intensity of physical activity is a predictor of femoral neck
strength, although it does not fully account for the greater bone
strength in boys. “Daily vigorous physical activity for at least
approximately 25 minutes seems to improve femoral neck bone health
in children.”
Basis for Study/Article This study from Portugal examined
whether the intensity and duration of physical activity affected
femoral neck strength and the bone mineral density of the femoral
neck, lumbar spine and total body in children.
Detailed Summary of Study DEXA scans were done in
143 girls and 150 boys (mean age 9.7 years), and their physical
activity was assessed using accelerometry. Compressive, bending and
impact strengths were calculated.
Results/Body Gender differences of 9% for
compressive strength, 10% for bending strength and 9% for impact
strength were found. Vigorous physical activity was “the main
physical activity predictor of femoral neck strength but did not
explain gender differences.” The most active boys (top 50%) had
higher values on all the strength ratings than the least active
(bottom 25%) boys. In girls, the only difference between the most
active (top 25%) and least active (bottom 25%) groups was bending
strength. Physical activity did not affect lumbar spine strength.
Sources & Other Links Sardinha LB, et al.
Objectively measured physical activity and bone strength in
9-year-old boys and girls. Pediatrics.
2008 Sep;122(3):e728-36.
Article Link (NCBI)
- ON
SCREENING COLONOSCOPY, BLACK PATIENTS HAVE HIGHER RISK OF POLYPS
>9 mm
Summary This multicenter
study found that on screening colonoscopy of asymptomatic patients,
the prevalence of polyps larger than 9 mm is 7.7% in black patients
vs. 6.2% in white patients. Although the prevalence of proximal
polyps <9 mm was similar between the races, the incidence was higher
in blacks older than 60.
Basis for Study/Article Black patients have a higher
incidence of colorectal cancer and a higher mortality rate. This
trial compared screening colonoscopy findings in asymptomatic black
vs. white patients.
Detailed Summary of Study The study comprised 80,061
white patients and 5,464 black patients undergoing screening
colonoscopy at 67 adult GI practice sites. The prevalence and
location of polyps larger than 9 mm were recorded.
Results/Body The prevalence of polyps larger than 9
mm was 7.7% in black patients vs. 6.2% in white patients; adjusted
odds ratios were 1.16 for black men and 1.62 for black women. The
prevalence of proximal polyps <9 mm was similar between the groups,
but they were more common in black patients older than 60.
Sources & Other Links Lieberman DA, et al.
Prevalence of colon polyps detected by colonoscopy screening in
asymptomatic black and white patients. JAMA.
2008;300(12):1417-22.
Article Link (NCBI)
- FDA APPROVES
UPDATED LABELING FOR PSORIASIS DRUG RAPTIVA
Safety
concerns drove labeling changesThe U.S. Food and
Drug Administration today announced labeling changes, including a
Boxed Warning, to highlight the risks of life-threatening
infections, including progressive multifocal leukoencephalopathy (PML),
with the use of Raptiva (efalizumab). The labeling changes are based
on the FDA's post-market surveillance. The FDA is also requiring the
submission of a Risk Evaluation and Mitigation Strategy (REMS),
which will include a Medication Guide for patients and a timetable
for assessment of the REMS.
Raptiva is a once-weekly injection approved for adults with
moderate to severe plaque psoriasis who are candidates for systemic
(whole body) therapy or phototherapy to control their psoriasis.
The FDA's Office of Surveillance and Epidemiology, charged by the
Agency with monitoring drugs once approved for the marketplace, has
received reports of serious infections leading to hospitalizations,
and deaths in some cases, in patients using Raptiva.
The now-required Boxed Warning will highlight the risk of
bacterial sepsis, viral meningitis, invasive fungal disease,
progressive multifocal leukoencephalopathy and other opportunistic
infections.
Additionally, Raptiva's label will be updated to include data
from juvenile animal studies in mice (age equivalent to a 1-14 year
old human). These data indicate a potential risk for the permanent
suppression of the immune system with repeat administration of
Raptiva in this age group. Raptiva is not approved for children
under 18 years of age.
"As part of FDA's monitoring of the life-cycle of approved
products, the agency received reports of serious infections in some
patients taking Raptiva. These reports led to our decision to
highlight these risks in the drugs labeling," said Janet Woodcock,
the FDA's director of the Center for Drug Evaluation and Research.
"Doctors and other prescribers should carefully evaluate and weigh
the risk/benefit profile of Raptiva for patients who would be more
susceptible to these risks."
Raptiva works by suppressing the immune system to reduce
psoriasis flare-ups, however by suppressing the body's natural
defense system, it can also increase the risk of serious infections
and malignancies in patients.
Patients identified to begin therapy with Raptiva should have
received all their age-appropriate vaccinations before starting the
drug. Vaccinations should not be administered to patients taking
Raptiva because immunity to the vaccination virus may not be
conferred.
Patients taking Raptiva should be educated about recognizing the
signs and symptoms of infection, PML (confusion, dizziness or loss
of balance, difficulty talking or walking, and vision problems),
anemia (dizziness upon standing, weakness or jaundice),
thrombocytopenia (bruising, bleeding gums, pin-point sized red or
purple dots under the skin), or the worsening of their psoriasis or
arthritis. Signs of a nervous system disorder include sudden onset
of numbness, tingling or weakness in the arms, legs or face.
If any of these signs appear, Raptiva patients should seek
immediate medical attention. Patients with pre-existing infections
or who have a compromised immune system should notify their health
care professional before beginning treatment with Raptiva.
Because reports of these adverse events were received voluntarily
from populations of unknown size, it is not always possible to
reliably estimate their frequency or establish a causal relationship
to the drug's use.
One report of PML in a Raptiva-treated patient came from an
ongoing post-marketing epidemiological study of patients with
psoriasis.
Health care professionals should monitor patients treated with
Raptiva for the signs and symptoms of these adverse events and also
instruct patients to report any such signs and symptoms to them
without delay.
Consumers and health care professionals can report adverse events
to the FDA's MedWatch program at 800-FDA-1088, by mail at MedWatch,
HF-2, FDA, 5600 Fishers Lane, Rockville, MD 20852-9787, or online at
www.fda.gov/medwatch/report.htm.
Raptiva was approved in 2003. It is manufactured by Genentech,
Inc. of San Francisco, Calif.
- SEQUENTIAL
THERAPY MAY BE EFFECTIVE FOR DRUG-RESISTANT H. PYLORI
Summary Sequential therapy consisting of 10 days of a
PPI, with amoxicillin for the first 5 days and clarithromycin and
tinidazole for the second 5 days, may be an effective way to treat
infection with H. pylori, which
is increasingly becoming resistant to standard medications.
Basis for Study/Article This article examines the
effectiveness of various treatment strategies for
H. pylori infection, given that
“the rate of treatment failure associated with established drug
regimens has increased at a rapid rate.”
Detailed Summary of Study
H. pylori is becoming increasingly resistant to
clarithromycin and metronidazole. The authors reviewed the
effectiveness of standard regimens vs. sequential therapy for
H. pylori infection.
Results/Body A large recent U.S. randomized
trial showed that “triple therapy” (7 to 10 days of a PPI
plus clarithromycin and amoxicillin) has an
H. pylori eradication rate of 78%.
The eradication rate for “quadruple therapy” (bismuth, metronidazole,
tetracycline, and a PPI) was 87.7% in a 1999 study, before
resistance became widespread. In contrast, sequential therapy—10
days of a standard-dose PPI b.i.d., with amoxicillin (1 g b.i.d.)
for the first 5 days and clarithromycin (500 mg b.i.d.) and
tinidazole (500 mg b.i.d.) for the second 5 day—showed higher
eradication rates in several studies, with acceptable adherence
rates. It was even effective in patients with infection that was
resistant to clarithromycin. The authors also discuss the limited
role of treatment with levofloxacin and rifabutin.
Sources & Other Links Vakil N, et al. Sequential
therapy for Helicobacter pylori:
time to consider making the switch? JAMA.
2008 Sep 17;300(11):1346-7.
-
IN OLDER WOMEN,
HOSPITALIZATION FOR NONSPECIFIC CHEST PAIN DOUBLES RISK FOR CAD
EVENT
Summary In
postmenopausal women, hospital admission for nonspecific chest pain
doubles the risk for a coronary artery disease event in the next 5
to 7 years. These women are “candidates for aggressive risk factor
treatment.” Hormone replacement therapy does not affect the risk of
either hospitalization for nonspecific chest pain or a subsequent
CAD event.
Basis for Study/Article The authors explored whether
being hospitalized for nonspecific chest pain is associated with a
woman’s risk of suffering a CAD event.
Detailed Summary of Study This study comprised 9,427
women in the Women’s Health Initiative Estrogen-Alone study
(follow-up, 7.1 years) and 15,105 women in the Women’s Health
Initiative Estrogen Plus Progestin trial (follow-up, 5.6 years).
They were postmenopausal (age 50 to 79) and did not have
cardiovascular disease at baseline. Hospital admissions for
nonspecific chest pain and subsequent CAD events were recorded.
Results/Body 322 women in the Estrogen-Alone study
and 249 in the Estrogen Plus Progestin trial were hospitalized for
nonspecific chest pain. They had double the risk of subsequent
nonfatal CAD events, including nonfatal MI (2.3% vs. 1.7%; hazard
ratio 2.1), revascularization (3.5% vs. 2.6%; hazard ratio 1.99),
and hospitalization for angina (3.7% vs. 2.3%; hazard ratio 2.39).
Sources & Other Links Robinson JG, et al.
Cardiovascular risk in women with nonspecific chest pain (from the
Women’s Health Initiative Hormone Trials).
Am J Cardiol. 2008 Sep 15;102(6):693-9.
Article Link (NCBI)
- OTC COUGH
AND COLD MEDICINES - PRODUCT LABELS BEING MODIFIED TO STATE "DO NOT
USE" IN CHILDREN UNDER 4 YEARS OF AGE
MedWatch - The FDA Safety Information and Adverse Event Reporting
Program
FDA notified healthcare professionals and
consumers that the Consumer Healthcare Products Association (CHPA)
is voluntarily modifying the product labels for consumers of over
the counter (OTC) cough and cold medicines to state "do not use" in
children under 4 years of age. FDA supports CHPA members to help
prevent and reduce misuse and to better inform consumers about the
safe and effective use of these products for children. FDA continues
to assess the safety and efficacy of these products and to revise
its OTC list of approved ingredients and amounts for these
medicines. Parents and care givers should adhere to the dosage
instructions and warnings on the label that accompanies OTC cough
and cold medications before giving the product to children, and
should consult their healthcare professionals if they have any
questions or concerns.Read the entire 2008 MedWatch Safety
Summaries, including a link to the FDA Press Release regarding the
above issue at:
Snapshot as on GMT: Fri Oct 10 04:50:38 2008
- BRAIN
SEROTONIN TRANSPORTER BINDING VARIES WITH THE SEASONS
Summary Brain serotonin transporter binding varies with
the seasons, with higher levels during periods of less sunshine.
“Since higher serotonin transporter density is associated with lower
synaptic serotonin levels, regulation of serotonin transporter
density by season is a previously undescribed physiologic mechanism
that has the potential to explain seasonal changes in normal and
pathologic behaviors.”
Basis for Study/Article “Brain serotonin is involved
in the regulation of physiologic functions, such as mating, feeding,
energy balance, and sleep.” This study from Canada examined whether
brain serotonin transporter binding varies depending on the amount
of daily sunshine.
Detailed Summary of Study Regional serotonin
transporter binding potential values were obtained from 88
drug-naďve healthy volunteers by PET scanning over 4 years. Levels
were then correlated with sunshine levels.
Results/Body Serotonin transporter binding levels
were higher in all brain regions scanned during the fall and winter,
when there was less sunlight.
Sources & Other Links Praschak-Rieder N, et al.
Seasonal variation in human brain serotonin transporter binding.
Arch Gen Psychiatry. 2008
Sep;65(9):1072-8.
Article Link (NCBI)
-
SURGERY VERSUS PRIMARY ENDOCRINE THERAPY FOR
OPERABLE PRIMARY BREAST CANCER IN ELDERLY WOMEN (70 YEARS PLUS)
Authors Hind Daniel, Wyld Lynda, Beverley Catherine,
Reed Malcolm W
Review Group Cochrane Breast Cancer GroupAbstract
Several studies have evaluated the clinical effectiveness of
endocrine therapy alone in women aged 70 years or over and who are
fit for surgery. ObjectivesTo identify and
review the evidence from randomised trials comparing primary
endocrine therapy (endocrine therapy alone) to surgery, with or
without adjuvant endocrine therapy, in the management of women aged
70 years or over with operable breast cancer.
Search strategy For this update, the Cochrane Breast Cancer
Group Specialised Register was searched 13th November 2007 using the
codes for "early breast cancer", "endocrine therapy", "psychosocial"
or "surgery". Selection criteria
Randomised trials comparing primary endocrine therapy with surgery,
with or without adjuvant endocrine therapy, in the management of
women aged 70 years or over with early breast cancer and who are fit
for surgery.Data collection and analysis Studies were assessed for
eligibility and quality, and data from published trials were
extracted by two independent reviewers. Hazard ratios were derived
for time-to-event outcomes, where possible, and a fixed-effect model
was used for meta-analysis. Toxicity and quality-of-life data were
extracted, where present. Where outcome data were not available,
trialists were contacted and unpublished data requested.Main
resultsSeven eligible trials were identified of which six had
published time-to-event data and one was published only in abstract
form with no usable data. The quality of the allocation concealment
was adequate in three studies and unclear in the remainder. In each
case the endocrine therapy used was tamoxifen.Data, based on an
estimated 869 deaths in 1571 women, were unable to show a
statistically significant difference in favour of either surgery or
primary endocrine therapy in respect of overall survival. However,
there was a statistically significant difference in terms of
progression-free survival, which favoured surgery with or without
endocrine therapy.The hazard ratios (HR) for overall survival were:
0.98 (95% confidence interval (CI) 0.74 to 1.30, P value 0.9) for
surgery alone versus primary
endocrine therapy; 0.86 (95% CI 0.73 to 1.00, P value 0.06)
for surgery plus endocrine therapy versus primary endocrine therapy.
The HRs for progression-free survival were: 0.55 (95% CI 0.39 to
0.77, P value 0.0006) for surgery alone versus primary endocrine
therapy; 0.65 (95% CI 0.53 to 0.81, P value 0.0001) for surgery plus
endocrine therapy versus primary endocrine therapy (each comparison
based on only one trial). Tamoxifen-related adverse effects included
hot flushes, skin rash, vaginal discharge, indigestion, breast pain,
sleepiness, headache, vertigo, itching, hair loss, cystitis, acute
thrombophlebitis, nausea, and indigestion. Surgery-related adverse
effects included paresthesia on the ipsilateral arm and lateral
thoracic wall in those who had axillary clearance. One study
suggested that those undergoing surgery suffered more psychosocial
morbidity at three months postsurgery, although this difference had
disappeared by two years.Authors' conclusions Primary endocrine
therapy should only be offered to women with oestrogen receptor (ER)
positive tumours who are unfit for or who refuse surgery. In a
cohort of women with significant co-morbid disease and ER-positive
tumours it is possible that primary endocrine therapy may be a
superior option to surgery. Trials are needed to evaluate the
clinical effectiveness of aromatase inhibitors as primary therapy
for an infirm older population with ER-positive tumours.
Implications Primary endocrine therapy should only
be offered to women with ER-positive tumours who are unfit for, or
who refuse, surgery. In a cohort of women with reduced life
expectancy, due to significant co-morbid disease, and ER-positive
tumours, primary endocrine therapy may be an appropriate treatment
choice.
Citation Hind D, Wyld L, Beverley C, Reed MW.
Surgery versus primary endocrine therapy for operable primary breast
cancer in elderly women (70 years plus). Cochrane Database of
Systematic Reviews 2008, Issue 3. Art. No.: CD004272. DOI:
10.1002/14651858.CD004272.pub2.
-
IN OLDER WOMEN WITH OSTEOPOROSIS, TIBOLONE
REDUCES FRACTURE AND CANCER RISK BUT DOUBLES RISK OF STROKES
Summary In older women with osteoporosis, tibolone
reduces the risk of fracture, breast cancer, and colon cancer, but
it doubles the risk of stroke. Because of the increased risk of
stroke, this trial was stopped early.
Basis for Study/Article This study examined the
effects of tibolone, a synthetic hormone used in HRT, on the risk of
fractures, breast cancer, colon cancer, and CV disease in
postmenopausal women with osteoporosis.
Detailed Summary of Study 4,538 women age 60 to 85 (BMD
T-score of -2.5 or less at hip or spine, or T-score -2.0 or less and
radiographic evidence of vertebral fracture) were randomized to
receive tibolone (1.25 mg/day) or placebo. Annual spine radiographs
were taken to assess for vertebral fractures, and other fractures,
breast cancer, and CV events were also recorded over a median
follow-up of 34 months.
Results/Body The rate of vertebral fracture was
70/1,000 person-years in the tibolone group vs. 126 in the placebo
group (relative hazard 0.55), and the rate of nonvertebral fracture
was 122 vs. 166 (relative hazard 0.74). The tibilone group had lower
rates of invasive breast cancer (relative hazard 0.32) and colon
cancer (relative hazard 0.31). However, the rate of stroke in the
tibolone group was more than double that in the placebo group
(relative hazard 2.19), and because of this the study was stopped
early. The rate of CHD and VTE did not differ between the groups.
Sources & Other Links Cummings SR, et al. The
effects of tibolone in older postmenopausal women.
N Engl J Med. 2008 Aug
14;359(7):697-708.
Article Link (NCBI)
- COST-EFFECTIVENESS
OF PPI THERAPY ALONG WITH LOW-DOSE ASPIRIN DEPENDS ON PATIENT'S RISK
OF GI BLEEDING
Summary In patients at average risk for upper GI
bleeding, taking a PPI along with low-dose, long-term aspirin is
cost-effective if the drug is purchased OTC. At prescription cost,
it would be cost-effective only in patients at high risk for upper
GI bleeding.
Basis for Study/Article Because of
the risk of upper GI bleeding in patients taking long-term low-dose
aspirin for CV protection, proton pump inhibitors are often
prescribed as well. This study looked at the cost-effectiveness of
taking a PPI and low-dose aspirin vs. aspirin alone.Detailed
Summary of Study The authors created a statistical model
comparing the life-long costs of the two regimens. Variables tested
were patient age (range 50 to 80), risk for upper GI bleeding, PPI
effectiveness and PPI cost per year (range $250 to $1,400).
Results/Body In patients at average risk for upper
GI bleeding, taking a PPI along with aspirin was cost-effective in
terms of its cost per life-year saved if the drug was purchased OTC.
At prescription cost, it was cost-effective only in patients at high
risk for upper GI bleeding.
Sources & Other Links Saini S, et al. Cost-effectiveness
of proton pump inhibitor cotherapy in patients taking long-term,
low-dose aspirin for secondary cardiovascular prevention.
Arch Intern Med. 2008 Aug
11;168(15):1684-90.
Article Link (NCBI)
- TOPICAL
GABAPENTIN REDUCES PAIN IN WOMEN WITH VULVODYNIA
Summary Topical gabapentin significantly decreases pain
and improves sexual function in many women with vulvodynia.
Basis for Study/Article This
retrospective study assessed the role of topical gabapentin in the
treatment of vulvodynia.Detailed Summary of Study
The authors reviewed the outcomes of 51 women using 2% to 6% topical
gabapentin to treat vulvodynia (19 generalized, 32 localized). 35
women were available for evaluation after at least 8 weeks of
treatment.
Results/Body After treatment, the mean pain score
was reduced from 7.26 to 2.49 on a scale of 0 to 10. 28 of the 35
women had at least a 50% drop in pain scores. Sexual function
improved in 17 of the 20 evaluable women with localized vulvodynia.
14% of patients discontinued treatment.
Sources & Other Links Boardman L, et al. Topical
gabapentin in the treatment of localized and generalized vulvodynia.
Obstet Gynecol. 2008
Sep;112(3):579-85.
Article Link (NCBI)
- HIGH
VITAMIN D LEVELS PROTECT AGAINST TYPE 2 DIABETES
Summary This 22-year follow-up study showed that high
vitamin D levels protect against type 2 diabetes. The effect was
less marked in women, who as a group had lower vitamin D levels than
men.
Basis for Study/Article This study
from Finland examined whether high vitamin D levels decrease the
risk of developing type 2 diabetes.Detailed Summary of Study
The researchers combined and analyzed the data from two case-control
studies showing that high vitamin D levels protects against type 2
diabetes. Information on vitamin D levels was collected between 1973
and 1980 in subjects aged 40 to 74 year who did not have diabetes.
Cases of diabetes were then recorded over 22 years of follow-up.
Incidence rates were calculated based on the subject’s vitamin D
level at baseline.
Results/Body Men with the highest vitamin D levels
had a lower risk of type 2 diabetes (relative odds between highest
and lowest levels, 0.28). Overall, women had lower vitamin D levels
than men, and the relative odds for developing type 2 diabetes
between the highest and lowest levels was 1.14.
Sources & Other Links Knekt P, et al. Serum vitamin
D and subsequent occurrence of type 2 diabetes.
Epidemiology. 2008
Sep;19(5):666-71.
Article Link (NCBI)
- HOME
INTRAVENOUS ANTIBIOTICS FOR CYSTIC FIBROSIS
Authors Balaguer Albert, González de Dios Javier
Review Group Cochrane Cystic
Fibrosis and Genetic Disorders GroupAbstract
Background: Recurrent endobronchial infection in cystic fibrosis
(CF) requires treatment with intravenous antibiotics for several
weeks usually in hospital, affecting health costs and quality of
life for patients and their families. Objectives: To determine
whether home intravenous antibiotic therapy in CF is as effective as
inpatient intravenous antibiotic therapy and if it is preferred by
individuals or families or both. Search strategy: We searched the
Cochrane Cystic Fibrosis and Genetic Disorders Group Trials Register
comprising references identified from comprehensive electronic
database searches and handsearches of relevant journals and abstract
books of conference proceedings.Most recent search of the Group's
Trials Register: April 2008. Selection criteria: Randomized and
quasi-randomized controlled studies of intravenous antibiotic
treatment for adults and children with CF at home compared to in
hospital. Data collection and analysis: The authors independently
selected studies for inclusion in the review, assessed
methodological quality of each study and extracted data using a
standardised form. Main results: Seventeen studies were identified
by the searches. Only one study could be included which reported
results from 17 participants aged 10 to 41 years with an infective
exacerbation of Pseudomonas aeruginosa. All their 31 admissions (18
hospital and 13 at home after two to four days of hospital
treatment) were analysed as independent events. Outcomes were
measured at 0, 10 and 21 days after initiation of treatment. Home
participants underwent fewer investigations than hospital
participants (P < 0.002) and general activity was higher in the home
group. No significant differences were found for clinical outcomes,
adverse events, complications or change of intravenous lines,
or time to next admission. Home participants received less
low-dose home maintenance antibiotic.
Quality of life measures showed no significant differences
for dyspnoea and emotional state, but fatigue and mastery were worse
for home participants, possibly due to a higher general activity and
need of support. Personal, family, sleeping and eating disruptions
were less important for home than hospital admissions.
Home therapy was cheaper for families and the hospital.
Indirect costs were not determined.
Authors' conclusions: Current evidence is
restricted to a single randomized clinical trial. It suggests that,
in the short term, home therapy does not harm individuals, entails
fewer investigations, reduces social disruptions and can be
cost-effective. There were both advantages and disadvantages in
terms of quality of life. The decision to attempt home treatment
should be based on the individual situation and appropriate local
resources. More research is urgently required.
Implications The current evidence is too limited to draw
conclusions for practice. The limited evidence available is from
participants who commenced treatment in hospital and suggests that,
in the short term, home therapy is associated with less social
disruption and no serious adverse events. The decision to commence
home therapy should be based on the individual and be co-ordinated
from units with appropriate outpatient resources.
Citation Balaguer A, González de Dios J. Home
intravenous antibiotics for cystic fibrosis. Cochrane Database of
Systematic Reviews 2008, Issue 3. Art. No.: CD001917. DOI:
10.1002/14651858.CD001917.pub2.
- CLINICAL/DEMOGRAPHIC
DETAILS, TREATMENT HISTORY DOES NOT APPEAR TO HELP IN CHOOSING A
SECOND-LINE ANTIDEPRESSANT
Summary "Clinical, demographic, and treatment history
were of little value in recommending one medication vs. another as a
second-step treatment for major depressive disorder."
Basis for Study/Article This study
identified characteristics of patients who responded to a
second-line antidepressant after initial treatment with citalopram (Celexa®)
failed to produce remission of major depressive disorder.
Detailed Summary of Study The 41-center study comprised
727 patients age 18 to 75 with major depressive disorder that did
not remit with citalopram. The second-line treatments given were
sustained-release bupropion (Wellbutrin®; 150 mg/day, titrated to
400 mg/day), sertraline (Zoloft®; 50 mg/day, titrated to 200
mg/day), and extended-release venlafaxine (Effexor®; 37.5 mg/day,
titrated to 375 mg/day). Depressive symptoms were rated using 3
scales. Factors increasing and decreasing the odds of remission were
identified.
Results/Body Factors increasing the odds of
remission were white race, employed status, cohabiting or married
status, private insurance, no suicide attempts, and a prior response
to citalopram (including intolerance). Factors decreasing the odds
of remission were greater Axis I psychiatric disorder comorbidity
and concurrent substance abuse. Intolerance of the second-line
treatment was more likely in patients with suicide attempts or
intolerance to citalopram; it was less likely in Hispanics.
Sources & Other Links Rush AJ, et al. Selecting
among second-step antidepressant medication monotherapies:
predictive value of clinical, demographic, or first-step treatment
features. Arch Gen Psychiatry.
2008 Aug;65(8):870-80.
Article Link (NCBI)
- EATING
NUTS, CORN POPCORN, SEEDS DOESN'T APPEAR TO INCREASE THE INCIDENCE
OF DIVERTICULOSIS
Summary This long-term study found
that eating nuts, corn, popcorn and seeds doesn’t increase the
incidence of diverticulosis or diverticular disease. “The
recommendation to avoid these foods to prevent diverticular
complications should be reconsidered.”Basis for Study/Article
<> This large prospective study evaluated the traditional belief
that eating nuts, corn, popcorn and seeds can cause diverticular
disease.
Detailed Summary of Study Dietary and medical
information was collected over an 18-year period from 47,228 men
aged 40 to 75 (participants in the Health Professionals Follow-up
Study) who did not have diverticulosis, cancer or inflammatory bowel
disease at baseline.
Results/Body During follow-up there were 801 cases
of diverticulitis and 383 cases of diverticular bleeding. Men who
ate popcorn and nuts at least twice a week were less likely to have
diverticulitis than those who ate them less than once a month
(hazard ratios 0.72 for popcorn, 0.80 for nuts). No link was found
between corn consumption and diverticulitis or between nut, corn or
popcorn consumption and diverticular bleeding or uncomplicated
diverticulosis.
Commentary The tradition based medicine approach of
repeating this long standing “ wisdom” of avoiding various dietary
compounds to prevent diverticulitis has never been proven, but
continues to be popular folklore. This study doesn’t fully evaluate
this issue; but certainly calls it into question. Overall,
healthcare providers should not advise patients to make dietary
changes which are completely unsupported by facts.
Grant E. Fraser M.D.
MedAlert Editor
Sources & Other Links Strate LL, et al. Nut, corn,
and popcorn consumption and the incidence of diverticular disease.
JAMA. 2008 Aug 27;300(8):907-14.
Article Link (NCBI
- INFANT
FORMULA MANUFACTURED IN CHINA: HEALTH INFORMATION ADVISORY DUE TO
REPORTS OF POSSIBLE CONTAMNATION WITH MELAMINE
FDA issued a Health Information Advisory
to consumers and healthcare professionals regarding milk-based
infant formula manufactured in China. The Chinese manufactured
infant formula may be contaminated with melamine. Melamine
artificially increases the protein profile of milk and can cause
kidney diseases. Currently, no Chinese manufacturers of infant
formula have fulfilled the requirements to sell this product in the
United States. FDA officials are investigating whether or not infant
formula manufactured in China is being sold in specialty markets
which serve the Asian community. Caregivers should not feed infant
formula manufactured in China to infants and should replace any
product from China with an appropriate infant formula manufactured
in the United States. Individuals should contact their health care
professional if they have questions regarding their infant's health
or if they note changes in their infant's health status.
Read the entire 2008 MedWatch Safety Summary, including a link to
the FDA Health Information Advisory regarding the above issue:
http://www.fda.gov/medwatch/safety/2008/safety08.htm#formulaChina
or
Snapshot as on GMT: Mon Sep 15 06:40:39 2008
- TUMOR
NECROSIS FACTOR-ALPHA BLOCKERS: DELAYS IN DIAGNOSIS OF FUNGAL AND
OTHER OPPORTUNISTIC INFECTION
*Tumor necrosis factor-alpha blockers (TNF blockers),
Cimzia (certolizumab pegol), Enbrel (etanercept), Humira (adalimumab),
and Remicade (infliximab)* *Audience: *Rheumatological,
gastroenterological and infectious disease healthcare professionals.
FDA notified healthcare professionals that
pulmonary and disseminated histoplasmosis, coccidioidomycosis,
blastomycosis and other opportunistic infections are not
consistently recognized in patients taking tumor necrosis factor- blockers (TNF blockers). This has resulted in delays in appropriate
treatment, sometimes resulting in death. For patients taking TNF
blockers who present with signs and symptoms of possible systemic
fungal infection, such as fever, malaise, weight loss, sweats,
cough, dypsnea, and/or pulmonary infiltrates, or other serious
systemic illness with or without concomitant shock, healthcare
professionals should ascertain if patients live in or have traveled
to areas of endemic mycoses. For patients at risk of histoplasmosis
and other invasive fungal infections, clinicians should consider
empiric antifungal treatment until the pathogen(s) are identified.
blockers (TNF blockers). This has resulted in delays in appropriate
treatment, sometimes resulting in death. For patients taking TNF
blockers who present with signs and symptoms of possible systemic
fungal infection, such as fever, malaise, weight loss, sweats,
cough, dypsnea, and/or pulmonary infiltrates, or other serious
systemic illness with or without concomitant shock, healthcare
professionals should ascertain if patients live in or have traveled
to areas of endemic mycoses. For patients at risk of histoplasmosis
and other invasive fungal infections, clinicians should consider
empiric antifungal treatment until the pathogen(s) are identified.
Read the complete MedWatch 2008 Safety summary, including links to
the Information for Healthcare Professionals page, FDA press release
and previous MedWatch alert on these products, at:
www.fda.gov/medwatch/safety/2008/safety08.htm#TNF2
or
Snapshot as on GMT: Fri Sep 5 04:59:23 2008
- HIGH FISH OIL INTAKE REDUCES
ATHEROSCLEROSIS IN JAPANESE, JAPANESE-AMERICANS AND WHITE MEN
Summary Compared with Japanese-American and white men,
Japanese men in their forties have twice the level of marine-derived
omega-3 fatty acids and have the lowest levels of atherosclerosis.
Basis for Study/Article The authors compared the
intake and effects of marine-derived omega-3 fatty acids in
Japanese, Japanese-American and white men age 40 to 49.
Detailed Summary of Study Intake of marine-derived
omega-3 fatty acids, intima-media thickness of the carotid artery,
coronary artery calcification and serum fatty acids were assessed in
281 men born and living in Japan, 281 men born in Japan and living
in the U.S., and 306 white men born and living in the U.S. All were
age 40 to 49.
Results/Body The Japanese men had the lowest levels
of atherosclerosis; the level was similar in the other two groups.
The Japanese men also had double the level of marine-derived omega-3
fatty acids compared to the other two groups. The Japanese men had a
significant inverse association of fatty acids with intima-media
thickness that was not explained by traditional CV risk factors.
This association was not found in the other two groups.
Sources & Other Links Sekikawa A, et al.
Marine-derived omega-3 fatty acids and atherosclerosis in Japanese,
Japanese-American, and white men: a cross-sectional study.
J Am Coll Cardiol. 2008 Aug
5;52(6):417-24.
Article Link (NCBI)
- OBSTRUCTIVE
SLEEP APNEA WORSENS INSULIN RESISTANCE AND GLUCOSE TOLERANCE IN
POLYCYSTIC OVARY SYNDROME
Summary Sleep apnea worsens insulin resistance and
glucose tolerance in women with polycystic ovary syndrome.
Basis for Study/Article The authors
investigated whether obstructive sleep apnea, which has been linked
to metabolic dysfunction, affects insulin resistance and glucose
tolerance in women with polycystic ovary syndrome.Detailed
Summary of Study 52 women with PCOS and 21 women without
PCOS matched for age and BMI underwent an overnight sleep study and
a 75-g oral glucose tolerance test.
Results/Body 56% of the PCOS women and 19% of the
controls were found to have sleep apnea. Impaired glucose tolerance
and insulin resistance were more common in the women with PCOS and
sleep apnea vs. those with PCOS but without sleep apnea. “Insulin
resistance and glucose tolerance were highly correlated with the
presence and severity” of sleep apnea.
Sources & Other Links Tasali E, et al. Impact of
obstructive sleep apnea on insulin resistance and glucose tolerance
in women with polycystic ovary syndrome. J
Clin Endocrinol Metab. 2008 Jul 22.
Article Link (NCBI)
- ALOE VERA EFFECTIVE FOR THE
TREATMENT OF ORAL LICHEN PLANUS
Aloe Vera apears to be an effective, inexpensive,
well-tolerated treatment for oral lichen planus. Oral lichen
planus affects 1% to 2% of the populartion. Treatment options
inlcude stroids, tacrolimus, retinoids, Fifty-four (54)
- GROWTH
HORMONE REDUCES HIV-ASSOCIATED ABDOMINAL FAT ACCUMULATION
Summary This randomized controlled trial found that in
HIV-positive patients receiving antiretroviral therapy, low-dose
growth hormone reduces abdominal fat accumulation, truncal obesity,
triglycerides, and diastolic blood pressure, but 2-hour glucose
levels are increased.
Basis for Study/Article “Antiretroviral therapy can
be associated with visceral adiposity and metabolic complications,
increasing cardiovascular risk.” Because reduced secretion of growth
hormone has been proposed as a contributing factor, the authors
examined the effects of GH administration on “body composition,
glucose, and cardiovascular parameters” in this population.
Detailed Summary of Study 56 HIV-positive patients
with abdominal fat accumulation and reduced GH secretion were
randomized to receive subcutaneous GH (average dose 0.33 mg/day) or
placebo for 18 months. Outcomes were change in body composition (CT
and DEXA scans), glucose levels, IGF-1, blood pressure and lipids.
Results/Body Compared to the placebo group, the GH
group had significantly decreased visceral fat, truncal obesity,
triglycerides and diastolic blood pressure; however, their 2-hour
glucose levels on glucose tolerance testing increased. The number of
adverse events did not differ significantly (23% for GH, 28% for
placebo).
Sources & Other Links Lo J, et al. Low-dose
physiological growth hormone in patients with HIV and abdominal fat
accumulation: a randomized controlled trial.
JAMA. 2008 Aug 6;300(5):509-19.
Article Link (NCBI)
- FATAL
STROKES MORE COMMON IN PATIENTS WITH LOW VITAMIN D LEVELS
Summary In patients undergoing coronary angiography,
low vitamin D levels are predictive of fatal stroke. “Vitamin D
supplementation is a promising approach in the prevention of
strokes.”
Basis for Study/Article This European study
investigated whether vitamin D levels affect the risk for fatal
stroke.
Detailed Summary of Study Levels of 25(OH)D and
1,25(OH)2D were measured in patients referred for coronary
angiography (n = 3,299 and 3,315). Seasonal variations in vitamin D
levels were corrected for statistically. Fatal strokes (ischemic and
hemorrhagic) were recorded over a median follow-up of 7.75 years.
Results/Body During follow-up there were 42 fatal
strokes, and low levels of 25(OH)D and 1,25(OH)2D were both
independent predictors of fatal strokes. Patients who had a history
of cerebrovascular disease at baseline also had lower vitamin D
levels.
Sources & Other Links Pilz S, et al. Low vitamin D
levels predict stroke in patients referred to coronary angiography.
Stroke. 2008 Jul 17. [Epub ahead
of print]
Article Link (NCBI)
- LOW-ENERGY
FEMORAL SHAFT FRACTURES HAVE A DISTINCTIVE PATTERN IN ALENDRONATE
(Fosamax®)
USERS
Summary Low-energy femoral shaft
fractures have a distinctive pattern in patients who take
alendronate (Fosamax®).Basis for Study/Article
“Long-term alendronate use may overly suppress bone metabolism,
limiting repair of microdamage and creating risk for insufficiency
fractures.” The authors examined whether alendronate use changes the
patterns of low-energy femoral shaft fractures.
Detailed Summary of Study The authors examined the
records of 70 patients (59 women, 11 men; average age 74.7) admitted
to their institution with low-energy femoral shaft fractures.
Fracture patterns were compared between those taking alendronate (n
= 25) and those not taking it (n = 45).
Results/Body 19 (76%) of the alendronate patients
and only 1 of the non-alendronate group had “a simple, transverse
fracture with a unicortical beak in an area of cortical
hypertrophy.” Duration of use was 6.9 years for alendronate users
with this pattern vs. 2.5 years in alendronate users who did not;
only one of the patients with this pattern had been taking
alendronate for less than 4 years. The pattern “may result from
propagation of a stress fracture whose repair is retarded by
diminished osteoclast activity and impaired microdamage repair”
resulting from long-term alendronate use.
Sources & Other Links Neviaser AS, et al. Low-energy
femoral shaft fractures associated with alendronate use.
J Orthop Trauma. 2008
May-Jun;22(5):346-50.
Article Link (NCBI)
- COMPARING
LOW-CARBOHYDRATE, LOW-FAT, AND MEDITERRANEAN DIETS
Summary This 2-year trial found that “Mediterranean and
low-carbohydrate diets may be effective alternatives to low-fat
diets.” Physicians can use the particular strengths of the diets—the
low-carb diet reduced lipids and the Mediterranean diet offered
better glycemic control—to devise an effective plan for a specific
patient.
Basis for Study/Article The authors compared the
effects of the three diets in moderately obese patients.
Detailed Summary of Study 322 patients with a mean BMI of
31 (mean age 52, 86% men) were randomized to one of three diets:
low-fat, restricted-calorie; Mediterranean, restricted-calorie; or
low-carbohydrate, without calorie restrictions. Adherence rates,
food intake, weight loss and outcomes were recorded over 2 years.
Results/Body
<> Adherence rates were 95.4% at 1 year and 84.6% at 2 years.
Mean weight loss was 2.9 kg for the low-fat group, 4.4 kg for the
Mediterranean group and 4.7 kg for the low-carb group. In the 272
subjects who completed the intervention, the corresponding figures
were 3.3, 4.6 and 5.5 kg. The subjects on the Mediterranean diet had
the highest fiber intake and the highest ratio of monounsaturated to
saturated fats. The low-carb group had the lower intake of
carbohydrates and the highest intake of fat, protein and
cholesterol. The ratio of total cholesterol to HDL decreased by 20%
in the low-carb group and by 12% in the low-fat group. In the 36
diabetic patients, “changes in fasting plasma glucose and insulin
levels were more favorable” in the Mediterranean group than in the
low-fat group.
Sources & Other Links Shai I, et al. Weight loss
with a low-carbohydrate, Mediterranean, or low-fat diet.
N Engl J Med. 2008 Jul
17;359(3):229-41.ticle
Link (NCBI)
- VIVITRO
(Naltrexone) - SERIOUS INJECTION SITE
REACTIONS COULD OCCUR
MedWatch - The FDA Safety
Information and Adverse Event Reporting Program
FDA informed healthcare professionals of the risk of adverse
injection site reactions in patients receiving naltrexone.
Naltrexone is indicated for the treatment of alcohol dependence in
patients who are able to abstain from alcohol in an outpatient
setting prior to initiation of treatment. Naltrexone is administered
as an intramuscular gluteal injection and should not be administered
intravenously, subcutaneously, or inadvertently into fatty tissue.
Physicians should instruct patients to monitor the injection site
and contact them if they develop pain, swelling, tenderness,
induration, bruising, pruritus, or redness at the injection site
that does not improve or worsens within two weeks. Physicians should
promptly refer patients with worsening injection site reactions to a
surgeon. Read the FDA recommendations for healthcare professionals
to consider regarding the use of Naltrexone injection.
Read the entire MedWatch Safety Summary, including a link to the
FDA Drug Information Page regarding this issue at: http://www.fda.gov/medwatch/safety/2008/safety08.htm#naltrexone
or
Snapshot as on GMT: Wed Aug 13 04:52:34
2008
- ASTHMA
IS LESS COMON IN CHILDREN WITH H.PYLORI COLONIZATION
Summary Asthma and other allergy symptoms are less
common in children with H. pylori
colonization.
Basis for Study/Article The authors assessed whether
there is an association between childhood asthma and exposure to
H. pylori.
Detailed Summary of Study The authors used data from
7,412 subjects in the National Health and Nutrition Examination
Survey (1999-2000).
Results/Body “H. pylori
seropositivity was inversely associated with onset of asthma before
5 years and current asthma in children aged 3-13 years.” It was also
inversely related to recent wheezing, allergic rhinitis, dermatitis,
eczema or rash. “These findings indicate new directions for research
and asthma prevention.”
Commentary H. pylori infection is also likely a
marker for a “dirtier” environment growing up. Although this
association may indeed be causative, it would seem much more likely
that it is simply a marker for being exposed to many environmental
factors at an early age.
Grant E. Fraser, M.D.
MedAlert Editor
Sources & Other Links
<> Chen Y, et al. Helicobacter pylori
colonization is inversely associated with childhood asthma.
J Infect Dis. 2008 Aug
15;198(4):553-60.
Article Link (NCBI)
- SUMATRIPTAN/NAPROXEN
COMBINATION EFFECTIVE FOR EARLY MIGRAINE TREATMENT
Summary A fixed-dose combination of sumatriptan and
naproxen aborts migraine if taken within 1 hour of onset.
Basis for Study/Article The authors examined the
efficacy and safety of a fixed-dose combination of sumatriptan (85
mg) and naproxen (500 mg) for early treatment of migraine.
Detailed Summary of Study In two separate studies,
adult patients (n = 576 and 535) were randomized to take either the
sumatriptan/naproxen combination or placebo within 1 hour of
migraine onset, while the pain was still mild. Pain relief and
adverse events were recorded.
Results/Body 2 hours after dosing, 52% and 51% of
the sumatriptan/naproxen patients were pain-free vs. 17% and 15% of
the control group. In the sumatriptan/naproxen patients, pain relief
started as early as 30 minutes and lasted for 2 to 24 hours; they
also had fewer migraine-associated symptoms than the control group.
The most common adverse events were nausea (4% or less) and
dizziness (2% or less).
Sources & Other Links Silberstein S, et al.
Multimechanistic (sumatriptan-naproxen) early intervention for the
acute treatment of migraine. Neurology.
2008 Jul 8;71(2):114-21.
Article Link (NCBI)
- SIMVASTATIN
USED WITH AMIODARONE ALERT
The FDA is notifying the public of the risk of a rare condition of
muscle injury called rhabdomyolysis, which can lead to kidney
failure or death, when simvastatin is used with amiodarone. This
risk is dose-related and increases when a dose of simvastatin
greater than 20 mg per day is given with amiodarone. A revision of
the simvastatin labeling in 2002 described an increased risk of
rhabdomyolysis when amiodarone is taken with simvastatin doses
greater than 20 mg daily. However, the FDA continues to receive
reports of rhabdomyolysis in patients treated concurrently with
amiodarone and simvastatin, particularly with simvastatin doses
greater than 20 mg daily. Prescribers should be aware of the
increased risk of rhabdomyolysis when simvastatin is prescribed with
amiodarone, and they should avoid doses of simvastatin greater than
20 mg per day in patients taking amiodarone.
- AUGUST
2008 FDA PATIENT SAFETY NEWS VIDEO IS AVAILABLE
NOW
For more "FDA Patient Safety News",
visit http://www.fda.gov/psn.
Please send any comments, questions or suggestions about the program
to PSNews@fda.gov
- VIAPRO
375 MG CAPSULES - VOLUNTARY RECALL
DUE TO POTENTIAL HARMFUL ANALOG OF SILDENAFIL
MedWatch - The FDA Safety Information and Adverse Event Reporting
Program
EG Labs, LLC, notified consumers and healthcare professionals not
to buy or use Viapro 375 mg Capsules because one lot of the product
was found to contain a potentially harmful undeclared ingredient,
thio-methisosildenafil, an analog of sildenafil, a FDA approved
product used to treat erectile dysfunction in men to enhance sexual
performance. The undeclared ingredient may interact with nitrates
found in some prescription drugs (such as nitroglycerin) and can
lower blood pressure to dangerous levels. Consumers with diabetes,
high blood pressure, high cholesterol, or heart disease often take
products containing nitrates. Consumers who have this product should
discontinue using it and consult their healthcare professional if
they experience any problems that may be related to taking Viapro.
- ERYTHROPOIESIS
STIMULATING AGENTS; PROCRIT, EPOGEN, AND ARANESP, - FDA CLARIFIES
APPROVED CONDITIONS FOR USE OF ESAs IN PATIENT WITH CANCER- REVISES
DOSING DIRECTIONS
MedWatch - The FDA Safety
Information and Adverse Event Reporting Program
Amgen and FDA informed healthcare professionals of modifications
to certain sections of the Boxed Warnings, Indications and Usage,
and Dosage and Administration sections of prescribing information
for Erythropoiesis Stimulating Agents (ESAs). The changes clarify
the FDA-approved conditions for use of ESAs in patients with cancer
and revise directions for dosing to state the hemoglobin level at
which treatment with an ESA should be initiated. Additional
revisions to prescribing information that ESAs are not intended for
use in patients receiving myelosuppressive therapy when the expected
outcome is cure and when to initiate and discontinue ESA dosing will
be forthcoming. FDA continues to encourage healthcare professionals
to discuss with their patients before starting or continuing therapy
with ESAs, the benefits of treatment with ESAs and the potential and
demonstrated risks of ESAs for thrombovascular events, shortened
time to tumor progression or recurrence, and shortened survival
time.
Read the entire 2008 MedWatch Safety Summary, including a link to
the FDA's Follow Up to an Ongoing Safety Review regarding this issue
at:
http://www.fda.gov/medwatch/safety/2008/safety08.htm#ESA2
- VACCINES
FOR PREVENTING INFLUENZA IN HEALTHY CHILDREN
Authors Jefferson Tom, Rivetti Alessandro, Harnden
Anthony, Di Pietrantonj Carlo, Demicheli Vittorio
Review Group Cochrane Acute Respiratory Infections
Group
Abstract The consequences of influenza in children
and adults are mainly absenteeism from school and work. However, the
risk of complications is greatest in children and people over 65
years old. Objectives: To appraise all
comparative studies evaluating the effects of influenza vaccines in
healthy children; assess vaccine efficacy (prevention of confirmed
influenza) and effectiveness (prevention of influenza-like illness)
and document adverse events associated with influenza vaccines.
Search strategy: We searched the Cochrane Central Register of
Controlled Trials (CENTRAL) (The Cochrane Library 2007, issue 3);
OLD MEDLINE (1950 to 1965); MEDLINE (1966 to September 2007); EMBASE
(1974 to September 2007); Biological Abstracts (1969 to September
2007); and Science Citation Index (1974 to September 2007).Selection
criteria Randomized controlled trials (RCTs), cohort and
case-control studies of any influenza vaccine in healthy children
under 16 years of age. Data collection and
analysis : Two review authors independently assessed trial quality
and extracted data. Main results Fifty-one
studies with 294,159 observations were included. Sixteen RCTs and 18
cohort studies were included in the analysis of vaccine efficacy and
effectiveness. From RCTs, live vaccines showed an efficacy of 82%
(95% confidence interval (CI) 71% to 89%) and an effectiveness of
33% (95% CI 28% to 38%) in children older than two compared with
placebo or no intervention. Inactivated vaccines had a lower
efficacy of 59% (95% CI 41% to 71%) than live vaccines but similar
effectiveness: 36% (95% CI 24% to 46%). In children under two, the
efficacy of inactivated vaccine was similar to placebo. Variability
in study design and presentation of data was such that a
meta-analysis of safety outcome data was not feasible. Extensive
evidence of reporting bias of safety outcomes from trials of live
attenuated vaccines impeded meaningful analysis. Authors'
conclusions: Influenza vaccines are
efficacious in children older than two but little evidence is
available for children under two. There was a marked difference
between vaccine efficacy and effectiveness. No safety comparisons
could be carried out, emphasizing the need for standardization of
methods and presentation of vaccine safety data in future studies.
It was surprising to find only one study of inactivated vaccine in
children under two years, given current recommendations to vaccinate
healthy children from six months old in the USA and Canada. If
immunization in children is to be recommended as a public health
policy, large-scale studies assessing important outcomes and
directly comparing vaccine types are urgently required.
Implications National policies for the vaccination
of healthy young children are based on very little evidence.
Citation Jefferson T, Rivetti A, Harnden A, Di
Pietrantonj C, Demicheli V. Vaccines for preventing influenza in
healthy children. Cochrane Database of Systematic Reviews 2008,
Issue 2. Art. No.: CD004879. DOI: 10.1002/14651858.CD004879.pub3.
- IN
SCIATICA, EARLY SURGERY HAS SHORT-TERM BUT NOT LONG-TERM BENEFITS
OVER CONSERVATIVE CARE
Summary For sciatica due to lumbar disc herniation,
this randomized controlled trial found that early surgery has
short-term but not long-term benefits over conservative
treatment.
Basis for Study/Article The authors of this
multi-center Dutch trial compared early surgery vs. prolonged
conservative treatment for sciatica.
Detailed Summary of Study Of
283 patients who had sciatica for 6 to 12 weeks, 141 were
assigned to early surgery (89% had microdiscectomy) and 142 were
assigned to 6 months of conservative treatment, with surgery if
needed (44% of them eventually had surgery). Pain was assessed
over 2 years of follow-up.
Results/Body Disability scores did not differ
between the groups over 2 years. Leg pain improved more quickly
in the early surgery group, but the difference was no longer
significant by 6 months and continued to decrease over 2 years.
Patient satisfaction fell slightly between 1 and 2 years; after
2 years 20% of patients reported an unsatisfactory outcome.
Sources & Other Links Peul WC, et al. Prolonged
conservative care versus early surgery in patients with sciatica
caused by lumbar disc herniation: two-year results of a
randomised controlled trial. BMJ.
2008 Jun 14;336(7657):1355-8.
Article Link (NCBI)
- DIABETES
INCREASES RISK OF HEARING LOSS
Summary Diabetes is an independent risk factor for
hearing loss.
Basis for Study/Article The authors
compared the prevalence of hearing impairment in adults with and
without diabetes.Detailed Summary of Study As part
of the National Health and Nutrition Examination Survey, information
was collected from 5,140 subjects (399 with type 1 or 2 diabetes)
age 20 to 69 who underwent audiometry.
Results/Body The age-adjusted prevalence of at least
mild low- or mid-frequency hearing loss was 21.3% in the diabetics
vs. 9.4% in those without diabetes (adjusted odds ratio 1.82). The
figures for high-frequency hearing loss were 54.1% vs. 32.0%
(adjusted odds ratio 2.16). The higher figures for diabetics were
not explained by risk factors for hearing loss such as noise
exposure, ototoxic medication use or smoking.
Sources & Other Links Bainbridge KE, et al. Diabetes
and hearing impairment in the United States: audiometric evidence
from the National Health and Nutrition Examination Survey, 1999 to
2004. Ann Intern Med. 2008 Jul
1;149(1):1-10.
Article Link (NCBI)
- SAFETY
REVIEW ERYTHROPOIESIS-STIMULATING AGENTS (ESAs)
EPOETIN ALFA (marketed as Procrit, Epogen)
DARBEPOETIN ALFA (marketed as Aranesp)
On April 22, 2008, FDA notified the manufacturer of Epogen/Procrit
and Aranesp of its decision to require additional safety-related
changes to the labeling for these products.
Amgen submitted labeling supplements for Epogen/Procrit
and Aranesp on May 22, 2008, following the March 13, 2008 Oncologic
Advisory Committee’s recommendations to make additional
safety-related changes to the labeling for these products. Amgen and
FDA have agreed on many of these changes, including to replace the
existing Patient Package Insert with a Medication Guide and to
modify certain sections of the Boxed Warnings, Indications and
Usage, and Dosage and Administration sections of package insert.
These changes are intended to clarify the FDA-approved conditions
for use of ESAs in patients with cancer and revise directions for
dosing to state the hemoglobin level at which treatment with an ESA
should not be initiated. While agreement was reached on the general
concepts, Amgen and FDA have not reached agreement on specific
wording on two points, including a warning statement that ESAs are
not intended for use in patients receiving myelosuppressive therapy
when the expected outcome is cure and statements regarding when to
initiate and to discontinue ESA dosing. Labeling discussions
concluded on July 15 and FDA issued a letter ordering the additional
changes on July 30, 2008.
FDA’s action to require these safety labeling changes follows the
completion of the review of information received in November 2007
and December 2007 and are in keeping with the recommendations made
at the March 13, 2008 Oncologic Drugs Advisory Committee meeting.
Amgen has been ordered to make the additional changes under new
authorities provided in the FDA Amendments Act of 2007 and has 5
days to appeal or 15 days to submit a supplement containing the
labeling changes.
FDA continues to encourage healthcare professionals to discuss
with their patients before starting or continuing therapy with ESAs,
the benefits of treatment with ESAs and the potential and
demonstrated risks of ESAs for thrombovascular events, shortened
time to tumor progression or recurrence, and shortened survival
time.
The FDA urges healthcare professionals to promptly report serious
and unexpected adverse reactions associated with Epogen, Procrit and
Aranesp to the FDA MedWatch reporting program, as described below.
Online
at
www.fda.gov/medwatch/report.htm
-
DIETARY ADVICE IN
PREGNANCY FOR PREVENTING GESTATIONAL DIABETES
Authors Tieu Joanna, Crowther
Caroline A, Middleton Philippa
Review Group Cochrane Pregnancy and Childbirth Group
Abstract Gestational diabetes mellitus (GDM) is a
form of diabetes that occurs during pregnancy which can result in
significant adverse outcomes for mother and child both in the short
and long term. The potential for adverse outcomes, in addition to
the increasing prevalence of gestational diabetes worldwide,
demonstrates the need to assess strategies, such as dietary advice,
that might prevent gestational diabetes.ObjectivesTo assess the
effects of dietary advice in preventing gestational diabetes
mellitus.Search strategy. We searched the Cochrane Pregnancy and
Childbirth Group's Trials Register (January 2008) and reference
lists of retrieved articles.Selection criteria Quasi-randomised and
randomised studies of dietary intervention for preventing glucose
intolerance in pregnancy.Data collection and analysis: Two review
authors independently conducted data extraction and quality
assessment. We resolved disagreements through discussion or through
a third author.Main resultsThree trials (107 women) were included in
the review. One trial (25 pregnant women) analysed high-fibre diets
with no included outcomes showing statistically significant
differences. Two trials (82 pregnant women) assessed low glycaemic
index (LGI) versus high glycaemic index diets for pregnant women.
Women on the LGI diet had fewer large for gestational age infants
(one trial; relative risk (RR) 0.09, 95% confidence interval (CI)
0.01 to 0.69), infants with lower ponderal indexes (two trials;
weighted mean difference (WMD) -0.18, 95% CI -0.32 to -0.04,
random-effects analysis) and lower maternal fasting glucose levels
(two trials; WMD -0.28 mmol/L 95% CI -0.54 to -0.02, random-effects
model). Results for women on the LGI diet on neonatal birth weight
were not conclusive under a random-effects model (two trials; WMD
-527.64 g, 95% CI -1119.20 to 63.92); however, on a fixed-effect
model, women on the LGI diet gave birth to lighter babies (two
trials; WMD -445.55 g, 95% CI -634.16 to -256.95). High
heterogeneity was observed between the trials in most results and
both were relatively small trials. One of these trials also included
a standard exercise regimen for all participants.Authors'
conclusionsWhile a low glycaemic index diet was seen to be
beneficial for some outcomes for both mother and child, results from
the review were inconclusive. Further trials with large sample sizes
and longer follow up are required to make more definitive
conclusions. No conclusions could be drawn from the high-fibre
versus control-diet comparison since the trial involved did not
report on many of the outcomes we prespecified.
Implications Overall,
results were inconclusive due to the limited number of trials,
participants and data provided in addition to high heterogeneity
between trials. While the results were promising, the evidence is
not sufficient to change clinical practice without further research
on dietary intervention for the prevention of gestational diabetes
mellitus (GDM) and its associated outcomes. One study in Australia
suggests that dietary advice for low and high GI diets can be
acceptable and affordable for women.
Citation Tieu J, Crowther CA, Middleton P. Dietary
advice in pregnancy for preventing gestational diabetes mellitus.
Cochrane Database of Systematic Reviews 2008, Issue 2. Art. No.:
CD006674. DOI: 10.1002/14651858.CD006674.pub2.
-
FDA ALERT
[7/24/2008]:
ABACAVIR (MARKETED AS ZIAGEN) AND
ABACAVIR-CONTAINING MEDICATIONS
Serious and sometimes fatal hypersensitivity
reactions (HSR) caused by abacavir therapy are significantly
more common in patients with a particular human leukocyte
antigen (HLA) allele, HLA-B*5701. Abacavir HSR is a multi-organ
syndrome characterized by 2 or more clinical signs or symptoms
that can include fever, rash, gastrointestinal symptoms,
respiratory symptoms and constitutional symptoms.
FDA has
reviewed data from 2 studies that support the recommendation for
pre-therapy screening for the presence of the HLA-B*5701 allele
and the selection of alternative therapy in positive subjects.
Genetic tests for HLA-B*5701 are already available and all
patients should be screened for the HLA-B*5701 allele before
starting or restarting treatment with abacavir or abacavir-containing
medications. Avoidance of abacavir therapy in HLA-B*5701
positive patients will significantly decrease the risk of
developing clinically-suspected abacavir HSR. For HLA-B*5701-positive
patients, treatment with an abacavir-containing regimen is not
recommended and should be considered only under exceptional
circumstances when the potential benefit outweighs the risk.
Development of clinically-suspected abacavir HSR requires
immediate and permanent discontinuation of abacavir therapy in
all patients, including patients negative for HLA-B*5701. This
new safety information will be reflected in updated product
labeling.www.fda.gov/medwatch/report/hcp.htm
- PREDICTING ELDERLY WOMEN AT HIGH V S. LOW RISK
FOR OSTEOPOROTIC FRACTURE
Summary A
low ultrasound bone stiffness index at the heel and four clinical
risk factors (age, history of fracture, recent fall, “failed chair
test”) can be used together to predict which elderly women are at
high risk for osteoporotic fracture.
Basis for Study/Article The authors of this Swiss
study developed and tested a predictive rule to identify elderly
women at high vs. low risk for osteoporotic fracture.
Detailed Summary of Study The authors used data from
a prospective multicenter study (6,174 women age 70 to 85) assessing
the predictive value of an ultrasound bone stiffness index at the
heel. Statistical analysis was used to identify additional factors
that were predictive of fracture.
Results/Body Risk factors for osteoporotic fracture
were age >75 years, low stiffness index in the heel, history of
fracture, a recent fall and “a failed chair test” (inability to rise
from a chair three times in a row without using the arms). A scoring
system incorporating these risk factors assigned 1,464 women to a
low-risk group and 4,710 to a high-risk group. The rate of
osteoporotic fracture was 6.1% for the high-risk group and 1.8% for
the low-risk group. 90% of those who had an osteoporotic hip
fracture were in the high-risk group.
Sources & Other Links Guessous I, et al.
Osteoporotic fracture risk in elderly women: estimation with
quantitative heel US and clinical risk factors.
Radiology. 2008 Jul;248(1):179-84.
Article Link (NCBI)
- IN
NEWLY DIAGNOSED TYPE 2 DM, SHORT-TERM
INSULIN THERAPY OUTPERFORMS OVRAL HYPOGLYCEMICS
Summary In patients with newly diagnosed diabetes, this
randomized, multicenter trial found that short-term, intensive
insulin therapy results in better beta-cell function and longer
glycemic remission compared to oral hypoglycemics.
Basis for Study/Article This Chinese trial compared
the effectiveness of intensive insulin therapy vs. oral
hypoglycemics in terms of beta-cell function and diabetes remission
rates in newly diagnosed diabetics.
Detailed Summary of Study 382 patients ages 25 to 70
from 9 centers in China with a fasting plasma glucose level of 7.0
to 16.7 mmol/L were randomized to receive short-term therapy with
insulin (continuous infusion or multiple daily injections) or oral
hypoglycemics. Drug treatment was stopped after blood glucose levels
were normal for 2 weeks. Glucose tolerance tests were done and blood
glucose levels, insulin and proinsulin levels were measured at
baseline, immediately after therapy, and 1 year after therapy.
Results/Body Compared with the oral hypoglycemic
group, the patients who received early insulin treatment had
significantly higher remission rates at 1 year (51.1% for continuous
insulin, 44.9% for multiple daily insulin injections, 26.7% for oral
hypoglycemics). More of the insulin group patients achieved their
target blood glucose goals (97.1% of the continuous infusion group,
95.2% of the multiple injections group, 83.5% of the oral
hypoglycemic group), and in less time (4.0 days, 5.6 days, 9.3
days). Beta-cell function improvements persisted at 1 year in the
insulin group but declined significantly in the oral treatment
group.
Sources & Other Links Weng J, et al. Effect of
intensive insulin therapy on beta-cell function and glycaemic
control in patients with newly diagnosed type 2 diabetes: a
multicentre randomised parallel-group trial.
Lancet. 2008 May
24;371(9626):1753-60.
Article Link (NCBI)
- OLANZAPINE
(Zyprexa®) USEFUL IN TREATING ANOREXIA
NERVOSA
Summary In women with anorexia
nervosa, this controlled trial found that olanzapine (Zyprexa®)
promotes weight gain and reduces obsessive symptoms.
Basis for
Study/Article The authors tested the utility of the
atypical antipsychotic drug olanzapine in the treatment of women
with anorexia nervosa.
Detailed Summary of Study 34 women with anorexia
nervosa were randomized to receive day hospital treatment plus
either placebo or olanzapine (flexible dose). Weight and obsessive
symptoms were recorded at baseline and after 10 weeks of treatment.
Results/Body Compared with the placebo group, the
women taking olanzapine had a greater rate of weight gain, achieved
their target weight earlier and had fewer obsessive symptoms. There
were no differences in adverse events between the groups. The
authors recommend that a large multicenter trial be conducted.
Sources & Other Links Bissada H, et al. Olanzapine
in the treatment of low body weight and obsessive thinking in women
with anorexia nervosa: a randomized, double-blind,
placebo-controlled trial. Am J Psychiatry.
2008 Jun 16.
Article Link (NCBI)
- WHICH
PRESCHOOLERS WITH WHEEZE WILL DEVELOP PERSISTENT ASTHMA?
Summary Preschoolers with
exercise-induced wheeze and a history of atopic disorders are much
more likely to develop persistent asthma.
Basis for
Study/Article The authors identified predictors of
persistent asthma in preschoolers with wheeze.
Detailed Summary of Study Parents of preschoolers in
Manchester, England, received questionnaires asking about their
children’s respiratory symptoms five times between 1993 and 2004. At
baseline the 628 children were <5 years old. Follow-up was at least
6 years.
Results/Body 32% of the children had wheeze at
baseline and 27% had it at the second time point. Predictors of
persistent asthma were exercise-induced wheeze (odds ratio 3.94) and
a history of atopic disorders (odds ratio 4.44). Children with both
predictors had a 53.2% likelihood of developing asthma; the
likelihood was 10.9% if neither was present.
Sources & Other Links Frank PI, et al. Long term
prognosis in preschool children with wheeze: longitudinal postal
questionnaire study 1993-2004. BMJ.
2008 Jun 21;336(7658):1423-6.
Article Link (NCBI)
- OBSTRUCTIVE
SLEEP APNEA IS COMMON IN WOMEN WITH NOCTURIA
Summary Obstructive sleep apnea is common in women with
nocturia, and 88% of women with dilute nighttime urine have OSA. “We
should consider a diagnosis of OSA in all patients with nocturia,”
even those with daytime overactive bladder symptoms.
Basis for Study/Article The authors explored the
association between obstructive sleep apnea and nocturia in women
and tested urine samples to see whether urine concentration was
predictive for sleep apnea.
Detailed Summary of Study 21 women with nocturia (16
of them also had daytime overactive bladder) and 10 control subjects
completed nocturia questionnaires, underwent a home sleep study and
provided evening and morning urine samples.
Results/Body 17 of the 21 women with nocturia (81%)
were found to have sleep apnea (13 of the 16 with daytime overactive
bladder and 4 of the 5 without) vs. 4 of the control group. “The
presence of diluted nighttime urine in a patient with nocturia was
88% sensitive for the presence of OSA.”
Sources & Other Links Lowenstein L, et al. The
relationship between obstructive sleep apnea, nocturia, and daytime
overactive bladder syndrome in women. Am J
Obstet Gynecol. 2008 May;198(5):598.e1-5.
Article Link (NCBI)
- HAVING
1/2 TO 1
ALCOHOLIC DRINK PER DAY PROTECTS AGAINST HIP FRACTURE
Summary This meta-analysis found
that people who have 1/2 to 1 alcoholic drink per day have a lower
risk of hip fracture compared to nondrinkers and heavier drinkers.
Basis for Study/Article The authors performed a
literature review to assess the effects of moderate alcohol
consumption on bone density and the risk of osteoporotic hip
fracture.
Detailed Summary of Study Effect sizes were pooled
for hip fracture and bone density, and results were synthesized for
four outcomes: non-hip fracture, bone density loss over time, bone
response to estrogen replacement, and bone remodeling.
Results/Body People who had 1/2 to 1 alcoholic drink
per day had a lower risk of hip fracture compared to nondrinkers
(relative risk 0.80); the relative risk was 1.39 for those who had
more than 2 drinks a day. “A linear relationship existed between
femoral neck bone density and alcohol consumption,” but “a precise
range of beneficial alcohol consumption cannot be determined.”
Sources & Other Links Berg KM, et al. Association
between alcohol consumption and both osteoporotic fracture and bone
density. Am J Med. 2008
May;121(5):406-18.
Article Link (NCBI)
- ADVERSE
EVENTS ASSOCIATED WITH PCA AND INSULIN
PUMPS IN ADOLESCENTS
Summary Over a 10-year period, there
were 1,594 reports to the FDA of adverse events associated with
adolescents’ use of insulin pumps (including 13 deaths) and 53
reports of adverse events associated with patient-controlled
analgesia pumps. “Studies need to further identify safety problems
in this age group.”
Basis for Study/Article After
receiving five reports of deaths in adolescents associated with
insulin pumps in 2005, the FDA conducted an assessment of the safety
of insulin and PCA pumps in this population.
Detailed Summary of Study The authors reviewed
reports submitted to the FDA from 1996 through 2005 about adverse
events associated with use of insulin or PCA pumps by adolescents
(ages 12 to 21). Demographics, type of adverse event, outcomes and
contributing factors were analyzed.
Results/Body Over a 10-year period, there were 1,594
reports of adverse events associated with insulin pumps, including
13 deaths, 2 possible suicide attempts, and several reports of
apparently device-related hyperglycemia or hypoglycemia. Some of the
contributing factors were compliance problems, lack of education,
“sports-related activities” and “dropping or damaging the pump.” In
82% of the events the patient was hospitalized. There were 53
reports of adverse events associated with PCA pumps. In half the
patients received too much medication; “tampering and noncompliance
were evident in some cases.”
The authors suggest more studies on the safety of these devices
in adolescents.
Sources & Other Links Cope J, et al. Adolescent use
of insulin and patient-controlled analgesia pump technology: a
10-year Food and Drug Administration retrospective study of adverse
events. Pediatrics. 2008
May;121(5):e1133-8.
Article Link (NCBI)
- DIABETES MELLITUS TYPE 2 AND ITS DURATION AFFECT
COGNITIVE FUNCTION IN THE ELDERLY
Summary
This prospective study found that community-dwelling older adults
with diabetes mellitus type 2 and those with a longer duration of
diabetes have a higher risk for cognitive decline.
Basis for Study/Article The authors assessed whether
the presence of diabetes mellitus type 2 and its duration affect
cognitive function in elderly men and women.
Detailed Summary of Study General cognition and
verbal memory were assessed at baseline in 5,907 men (mean age 74.1)
in the Physicians’ Health Study II and 6,326 women (mean age 71.9)
in the Women’s Health Study. 553 men and 405 women had diabetes.
Follow-up assessments were made 2 years after baseline; the women
had a third assessment 4 years later.
Results/Body Diabetic subjects had significantly
lower baseline scores. A longer duration of diabetes was
significantly associated with lower scores at baseline and
follow-up. Diabetic men and women had significantly greater
cognitive decline at follow-up than those without diabetes.
Sources & Other Links Okereke OI, et al. Type 2
diabetes mellitus and cognitive decline in two large cohorts of
community-dwelling older adults. J Am
Geriatr Soc. 2008 Jun;56(6):1028-36.
Article Link (NCBI)
- HOME
BLOOD PRESSURE MEASUREMENT IS USEFUL AND SHOULD BE COVERED BY
INSURANCE
Summary Home blood pressure measurement is useful in
the management of hypertension and should be covered by medical
insurance.
Basis for Study/Article This is a scientific
statement from the American Hearth Association, the American Society
of Hypertension and the Preventive Cardiovascular Nurses
Association. The authors reviewed the evidence on the use of home
blood pressure monitoring by hypertensive patients and made
recommendations for such use.
Results/Body Home monitoring should be part of the
management regimen in all patients with known or suspected
hypertension. It can be useful in identifying “white-coat
hypertension.” Patients should use oscillometric monitors that
measure BP on the upper arm, and should be shown how to use them
properly. Target BP is <135/85, or <130/80 in high-risk patients.
Home monitoring “has the potential to improve the quality of care
while reducing costs and should be reimbursed.”
Sources & Other Links Pickering TG, et al. Call to
action on use and reimbursement for home blood pressure monitoring:
executive summary: a joint scientific statement from the American
Heart Association, American Society of Hypertension, and Preventive
Cardiovascular Nurses Association.
Hypertension. 2008 Jul;52(1):1-9.
Article Link (NCBI)
-
DISTINGUISHING ORGANIC VS. MECHANICAL LOW BACK PAIN IN CHILDREN
Summary
In children with
short-term symptoms, a bone scan is particularly useful n
distinguishing organic low back pain from mechanical back pain.
Basis for
Study/Article
The authors
identified "which combination of imaging modalities provides the
most sensitive and specific screening protocol for children with low
back pain."
Detailed Summary of
Study
The authors reviewed
the records of 100 children age 2 to 18 with low back pain without night
pain or constitutional symptoms, examining the utility of the imaging
studies that were done.
Results/Body
The hyperextension test
and on x-ray had a negative predicative value of 0.81 and a sensitivity
of 0.90. For children with non-neurologic symptoms of <6 weeks
duration, a bone scan had 100% negative predictive value and
sensitivity; it is "the most useful screening test because it is
accurate, accessible, inexpensive and unlikely to require sedation."
Mechanical back pain was most likely in children with painless
hyperextension and negative AP, lateral and oblique lumbar x-rays and
MRI.
Sources & Other
Links
Auerbach JD, et al,
Streamlining the evaluation of low back pain in children. Clin
Orthop Relat Res. 2008 June 16. Article-Link (NCBI)
-
ALPHA-LINOLENIC
ACID REDUCES RISK OF MYOCARDIAL INFARCTION
(HealthDay News) - Increased omega-3 fatty acid
alpha-linolenic acid (ALA) intake is associated with decreased
risk of non-fatal acute MI, according to a Harvard School of
Public Health case-control study of 1,819 patients with a 1st
non-fatal acute MI and 1,819 controls. In a separate
report, increased omega-6- fatty ALA intake is associated with
reduction in systolic and diastolic blood pressure, according to
a Japanese study of 2,238 patients without known cardiovascular
disease. Authors concluded that these results lend support
to current recommendations for increased ingestion of
polyunsaturated fatty acid from vegetable sources. (PubMed)
-
COFFEE RELATED TO A HEALTHIER HEART
Heavy coffee drinking may lower risk of cardiovascular death.
Summary: This long-term study found
that people who drink six or more cups of coffee each day have
lower risk of dying of cardiovascular disease.
The authors explored the association between
coffee and mortality (all-cause and disease-specific)
Detailed Summary of Study
As part of the prospective Health Professionals
Follow-up Study and the Nurses' health Study, information was
collected on self-reported coffee consumption and death rates
for cancer and cardiovascular disease, and was recorded.
The participants were 41,736 men and 86,214 women who did not
have cardiovascular disease or cancer at baseline.
Follow-up was 18 years in men and 24 years in women. The
six levels of coffee consumption were <1 cup per months, 1 cup
per months to 4 cups per week, 5 to 7 cups per week, 2 or 3 cups
a day, 4 or 5 cups a day and 6 or more cups a day.
At follow-up, 6,888 of
the men had dies (2,049 due to cardiovascular disease, 2,491 due to
cancer) and 11,095 of the women had died )2,368 due to cardiovascular
disease, 5,011 due to cancer). In men, the relative risks for
al-cause mortality were 1.0, 1.07, 1.02, 0.97, 0.93, and 0.80 for the
six levels of coffee consumption, after adjusting for age, smoking and
other risk factors for cancer and CVD. In women the figures were
1.0,0.98,0.3, 0.82, 0.74, and 0.83. Most of the effect was due to
a reduction in CVD mortality rather than cancer mortality.
"Decaffeinated coffee consumption was associated with a small reduction
in all-cause and CVD mortality."
Sources & Other
Links
Lopez-Garcia E, et al.
The relationship of coffee consumption with mortality. Ann Intern
Med. 2008 Jun 17;148(12):904-13
-
MEDICAL GRADE
HONEY; LAST RESORT FOR DRUG-RESISTANT INFECTIONS
In vitro studies of bactericidal activity show
that a 40% solution of of honey reproducibly killed all
bacterial isolates tested, including MRSA, vancomycin-resistant
E. faecium, and multidrung-resistant gram-negative rods.
42 healthy volunteers had small forearm patches of skin swabbed
with honey and covered with polyurethane dressings for 2 days.
Compared with control skin patches on the same volunteers,
honey-covered patches were culture-negative significatly more
often. Medical-grade honey is produced by bees in closed
greenhouses. Grocery-grade honey is not standardized and
can be bacterially contaminated. Medline (Journal Watch).
-
ANGINA PREVENTION
1
year
after MI, angina remains in 20% of patients
Summary
This multi-center study
found that 1 year after myocardial infarction, 20% of patients still
have angina. The most significant associated factors are
depressive symptoms, a history of CABG surgery, and a prior history of
angina.
Detailed Summary of
Study
Angina was assessed 1
year after MI in 1,957 patients at 19 hospitals. Information
was collected on demographics, clinical history, MI presentation and
inpatient and outpatient treatment.
Results/Body
19.5% of the patients
had angina 1 year after their MI. Associated factors were younger
age (relative risk per 10-year decrease, 1.19), nonwhite race/male
gender (relative risk 1.50), prior history of angina (1.78), CABG
(1.92), recurrent rest angina during hospital stay (1.54), continued
smoking after MI (1.23), history of revascularization after the first
hospitalization (1.37), and presence of new (1.96), persistent (1.88) or
transient (1.77) depressive symptoms.
Sources & Other
Links
Maddox TM, et al.
Angina at 1 year after myocardial infarction; prevalence and associated
findings. Arch Intern Med. 2998 Jun23;168(12);1310-6 Article
Link (NIBI)
-
AVASTIN (BEVACIZUMAB) AND SUNITINIB MALATE ASSOCIATED HEMOLYTIC
ANEMIA
Genentech, Inc. informed healthcare professionals of reports of
several cases of microangiopathic hemolytic anemia (MAHA) in
patients with solid tumors receiving Avastin in combination with
sunitinib malate. Avastin is not approved for use in combination
with sunitinib malate and this combination is not recommended.
Twenty-five patients were enrolled in a Phase I dose-escalation
study combining Avastin and sunitinib malate. The study consisted of
3 cohorts using a fixed dose of Avastin at 10 mg/kg/IV every 2 weeks
and escalating doses of sunitinib that included 25, 37.5, and 50 mg
orally daily given in a 4 weeks on/2 weeks off schedule. Five of 12
patients at the highest sunitinib dose level exhibited laboratory
findings consistent with MAHA. Two of these cases were considered
severe with evidence of thrombocytopenia, anemia, reticulocytosis,
reductions in serum haptoglobin, schistocytes on peripheral smear,
modest increases in serum creatinine levels, and severe
hypertension, reversible posterior leukoencephalopathy syndrome, and
proteinuria. The findings in these two cases were reversible within
three weeks upon discontinuation of both drugs without additional
interventions. Healthcare professionals should report cases of MAHA
or any serious adverse events suspected to be associated with the
use of Avastin
-
FDA PRELIMINARY PHN: POSSIBLE
MALFUNCTION OF ELECTRONIC MEDICAL DEVICES CAUSED BY COMPUTED
TOMOGRAPHY (CT) SCANNING
FDA informed healthcare professionals of the possibility that
x-rays used during CT examinations may cause some implanted and
external electronic medical devices to malfunction. Most
patients with electronic medical devices undergo CT scans
without any adverse consequences. However, the Agency has
received a small number of reports of adverse events in which CT
scans may have interfered with electronic medical devices,
including pacemakers, defibrillators, neurostimulators, and
implanted or externally worn drug infusion pumps. FDA is
continuing to investigate the issue and is working with the
manufacturer to raise awareness in the healthcare community. See
the FDA Public Health Notification for a description of adverse
event reports and recommendations regarding reducing the
potential risk to patients.
-
DIABETES TYPE 1 & 2 CONTROL VIA THE
DCCT AND UKPDS STUDIES-GROUND BREAKING HISTORY OF GLOBAL MEDICINE
REVIEW
The Diabetes Control and Complications Trial (DCCT) evaluated the
importance of strict glycemic control in patients. Groups were
originally (1993) divided into intensive therapy (average blood
glucose of 155 mg/dL) versus conventional therapy on long-term
microvascular complications in type 1 diabetes mellitus.
Compared to conventional therapy, the risk of development of
retinopathy declined by 76%, the risk of progression of retinopathy
even declined by 54%, the occurrence of microalbuminuria declined by
39%, the occurrence of overt proteinuria declined by 54%, and the
risk of development of neuropathy declined by 60% in the intensive
therapy group. The major adverse event was a 2-fold to 3-fold
increase in severe hypoglycemia. New England Journal Medicine
1993:329:977-986.
Similar to the DCCT, the United Kingdom Prospective Diabetes Study (UKPDS)
investigated the incidence of complications in groups receiving
intensive therapy versus conventional therapy in patients with type
2 diabetes. The intensive therapy group had a significant 25%
decrease in incidence of microvascular complications. Lancet
1998:352:837-852.
- BRIGHT LIGHT
MODESTLY IMPROVES FUNCTION IN ELDERLY INSTITUTIONALIZED PATIENTS
Summary The randomized controlled trial found that
exposure to bright light modestly improves function in
institutionalized elderly patients. Melatonin has an adverse effect
on function and should be used only in conjunction with bright light
therapy.
Basis for Study/Article Some of most troublesome
symptoms of dementia have been associated with circadian rhythm
disturbances. The authors explored whether bright light therapy and
melatonin, two purported circadian-rhythm synchronizers, could
improve the functioning of elderly patients living in institutions
in the Netherlands.
Detailed Summary of Study 189 patients (90% female,
87% with dementia, mean age 85.8 years) living in 12 institutions
were randomized to receive therapy with whole-day bright or dim
light or melatonin or placebo for a mean of 15 months. Cognitive and
noncognitive symptoms, ADLs and adverse effects were assessed every
6 months.
Results/Body Findings
showed that light therapy “has a modest benefit in improving some
cognitive and noncognitive symptoms of dementia.” It slightly
improved cognitive deterioration and depressive symptoms and slowed
the increase in functional limitations. Patients taking melatonin
fell asleep more quickly and slept longer, but melatonin also had an
adverse impact on both positive and negative affect; if given
without light therapy, it also increased withdrawn behavior. When
given together, light therapy and melatonin lessened aggressive
behavior, increased sleep efficiency and improved nocturnal
restlessness.
Sources & Other Links Riemersma-van der Leck RF,
Swaab DF, Twisk J, et al. Effect of bright light and melatonin on
cognitive and noncognitive function in elderly residents of group
care facilities: A randomized controlled trial.
JAMA. 2008;299(22):2642-2655.
- DIETARY
ADVICE IN PREGNANCY FOR PREVENTING GESTATIONAL DIABETES MELLITUS
Authors Tieu Joanna, Crowther Caroline A, Middleton
Philippa
Review Group Cochrane Pregnancy and Childbirth Group
Abstract Gestational diabetes mellitus (GDM) is a
form of diabetes that occurs during pregnancy which can result in
significant adverse outcomes for mother and child both in the short
and long term. The potential for adverse outcomes, in addition to
the increasing prevalence of gestational diabetes worldwide,
demonstrates the need to assess strategies, such as dietary advice,
that might prevent gestational diabetes. Objectives,
To assess the effects of dietary advice in preventing
gestational diabetes mellitus.
Search strategy. We searched the Cochrane Pregnancy and Childbirth
Group's Trials Register (January 2008) and reference lists of
retrieved articles. Selection
criteria Quasi-randomised and randomised studies of dietary
intervention for preventing glucose intolerance in pregnancy.Data
collection and analysis: Two review authors independently conducted
data extraction and quality assessment. We resolved disagreements
through discussion or through a third author.
Main results: Three trials
(107 women) were included in the review. One trial (25 pregnant
women) analysed high-fibre diets with no included outcomes showing
statistically significant differences. Two trials (82 pregnant
women) assessed low glycaemic index (LGI) versus high glycaemic
index diets for pregnant women. Women on the
LGI diet had fewer large for gestational age infants (one
trial; relative risk (RR) 0.09, 95% confidence interval (CI) 0.01 to
0.69), infants with lower ponderal indexes (two trials; weighted
mean difference (WMD) -0.18, 95% CI -0.32 to -0.04, random-effects
analysis) and lower maternal fasting glucose levels (two trials; WMD
-0.28 mmol/L 95% CI -0.54 to -0.02, random-effects model). Results
for women on the LGI diet on neonatal birth weight were not
conclusive under a random-effects model (two trials; WMD -527.64 g,
95% CI -1119.20 to 63.92); however, on a
fixed-effect model, women on the LGI diet gave birth to lighter
babies (two trials; WMD -445.55 g, 95% CI -634.16 to
-256.95). High heterogeneity was observed between the trials in most
results and both were relatively small trials. One of these trials
also included a standard exercise regimen for all participants.
Authors' conclusions:
While a low glycaemic index diet was seen to
be beneficial for some outcomes for both mother and child, results
from the review were inconclusive. Further trials with large
sample sizes and longer follow up are required to make more
definitive conclusions. No conclusions could be drawn from the high-fibre
versus control-diet comparison since the trial involved did not
report on many of the outcomes we prespecified.
Implications Overall, results were inconclusive due
to the limited number of trials, participants and data provided in
addition to high heterogeneity between trials.
While the results were promising, the evidence is not
sufficient to change clinical practice without further research on
dietary intervention for the prevention of gestational diabetes
mellitus (GDM) and its associated outcomes. One study in Australia
suggests that dietary advice for low and high GI diets can be
acceptable and affordable for women.
Citation Tieu J, Crowther CA, Middleton P. Dietary
advice in pregnancy for preventing gestational diabetes mellitus.
Cochrane Database of Systematic Reviews 2008, Issue 2. Art. No.:
CD006674. DOI: 10.1002/14651858.CD006674.pub2
- ANTIBIOTICS
FOR ACUTE MAXILLARY SINUSITIS
Authors Ahovuo-Saloranta Anneli, Borisenko Oleg V,
Kovanen Niina, Varonen Helena, Rautakorpi Ulla-Maija, Williams Jr
John W, Mäkelä Marjukka
Review Group Cochrane Acute Respiratory Infections
Group
Abstract Expert opinions vary on the appropriate
role of antibiotics for sinusitis, one of the most commonly
diagnosed conditions among adults in ambulatory care. Objectives: We
examined whether antibiotics are effective in treating acute
sinusitis, and if so, which antibiotic classes are the most
effective. Search strategy. We
searched the Cochrane Central Register of Controlled Trials
(CENTRAL) (The Cochrane Library, 2007, Issue 3); MEDLINE (1950 to
May 2007) and EMBASE (1974 to June 2007).
Selection criteria Randomized controlled trials (RCTs)
comparing antibiotics with placebo or antibiotics from different
classes for acute maxillary sinusitis in adults. We included trials
with clinically diagnosed acute sinusitis, whether or not confirmed
by radiography or bacterial culture. Data collection and analysis:
At least two review authors independently screened search results,
extracted data and quality assessed trials. Risk ratios (RR) were
calculated for differences in the intervention and control groups to
see whether or not the treatment was a failure. In meta-analysing
the placebo-controlled studies, the data across antibiotic classes
were combined. Primary outcomes were the clinical failure rates at 7
to 15 days and 16 to 60 days follow up. Main results:
Fifty-seven studies were included in the review; six
placebo-controlled studies and 51 studies comparing different
classes of antibiotics. Five studies involving 631 participants
provided data for comparison of antibiotics to placebo, when
clinical failure was defined as a lack of cure or improvement at 7
to 15 days follow up. These studies found a slight statistical
difference in favor of antibiotics, compared to placebo, with a
pooled RR of 0.66 (95% confidence interval (CI) 0.44 to 0.98).
However, the clinical significance of the result is equivocal, also
considering that cure or improvement rate was high in both the
placebo group (80%) and the antibiotic group (90%). Based on six
studies, when clinical failure was defined as a lack of total cure,
there was significant difference in favor of
antibiotics compared to placebo with a pooled RR of 0.74 (95%
CI 0.65 to 0.84) at 7 to 15 days follow up. None of the antibiotic
preparations was superior to each other.
Authors' conclusions:
Antibiotics have a small treatment effect in
patients with uncomplicated acute sinusitis in a primary care
setting with symptoms for more than seven days. However, 80% of
participants treated without antibiotics improve within two weeks.
Clinicians need to weigh the small benefits of antibiotic treatment
against the potential for adverse effects at both the individual and
general population level.
Implications Antibiotics cause a small treatment
effect in patients with uncomplicated acute sinusitis in a primary
care setting with symptoms for more than seven days. However, 80% of
patients treated with a placebo also improve within two weeks. The
clinician needs to weigh the moderate benefits of antibiotic
treatment against the potential for adverse effects at both the
individual and general population level.
Citation Ahovuo-Saloranta A, Borisenko OV, Kovanen
N, Varonen H, Rautakorpi UM, Williams Jr JW, Mäkelä M.
Antibiotics for acute maxillary sinusitis. Cochrane Database of
Systematic Reviews 2008, Issue 2. Art. No.: CD000243. DOI:
10.1002/14651858.CD000243.pub2.
- IS TYPE 2
DIABETES A RISK FACTOR FOR DEPRESSION?
Summary
Depressed people are slightly more likely to
develop type 2 diabetes, mostly because of lifestyle factors.
Conversely, depression was less common in people with impaired
fasting glucose levels and untreated type 2 diabetes than it was in
people with normal fasting glucose levels and those with treated
type 2 diabetes.
Basis for Study/Article “Depressive symptoms are
associated with development of type 2 diabetes, but it is unclear
whether type 2 diabetes is a risk factor for elevated depressive
symptoms.”
Detailed Summary of Study The researchers conducted
two analyses of data from the Multi-Ethnic Study of Atherosclerosis,
which comprised men and women age 45 to 84 who were enrolled in
2000-02 and followed up until 2004-05. The first analysis looked at
the incidence of type 2 diabetes in 5,201 subjects who did not have
diabetes at baseline, comparing the incidence in those with vs.
without depressive symptoms. The second analysis looked at the
incidence of depression in 4,847 subjects who were not depressed at
baseline, comparing the incidence in those with vs. without
diabetes. Depression was defined as use of antidepressants or a
score of  16 on
the Center for Epidemiologic Studies Depression Scale. Fasting
glucose levels were defined as normal (<100 mg/dL), impaired (100 to
125 mg/dL) or type 2 diabetes (either receiving treatment or
126 mg/dL). 16 on
the Center for Epidemiologic Studies Depression Scale. Fasting
glucose levels were defined as normal (<100 mg/dL), impaired (100 to
125 mg/dL) or type 2 diabetes (either receiving treatment or
126 mg/dL).
Results/Body In analysis 1, the incidence rate of
type 2 diabetes was 22.0 per 1,000 person-years for those with
depression and 16.6 for those without depression. This association
was partially explained by lifestyle factors. In analysis 2, the
incidence rate of depression was 36.8 per 1,000 person-years for
those with normal fasting glucose levels, 27.9 for those with
impaired levels, 31.2 for those with untreated diabetes and 61.9 for
those with treated diabetes. Odds ratios for developing depression,
compared to those with normal fasting glucose levels, were 0.79 for
those with impaired levels, 0.75 for those with untreated diabetes
and 1.54 for those with treated diabetes. The association remained
significant after adjusting for multiple factors.
Sources & Other Links Golden SH, et al. Examining a
bidirectional association between depressive symptoms and diabetes.
JAMA. 2008 Jun
18;299(23):2751-9.
Article Link (NCBI)
- H. PYLORI
INFECTIONS MAY TRIGGER SIDS
Summary This study from Norway found that
H. pylori infection is
significantly more common in SIDS victims and infants who die of
infection. The authors hypothesize that such infection “may be
involved as the triggering pathogen” for SIDS.
Basis for Study/Article The authors explored the
proposed link between H. pylori
infection and SIDS.
Detailed Summary of Study Immunoassay for the
H. pylori antigen was performed
in infants who died of various causes (122 SIDS victims; 17 infants
who died of infection; 11 accidental or violent deaths) and 156 live
controls.
Results/Body H. pylori
was found in stool samples of 25% of the SIDS victims (p <0.001 vs.
live controls), 53% of the babies who died of infection (p <0.001),
9% of accidental deaths (p = 0.6) and 8% of the live controls. In
infants ages 1 to 5 months of age, the classic age for SIDS, 21 of
the 67 SIDS victims tested positive for H.
pylori vs. only 1 of the 68 live controls. “We
hypothesize that H. pylori
infection in infancy may be involved as the triggering pathogen for
sudden death during the first five months after birth.”
Sources & Other Links Stray-Pederson A, et al.
Helicobacter pylori antigen in
stool is associated with SIDS and sudden infant deaths due to
infectious disease. Pediatr Res.
2008 Jun 4. [Epub ahead of print]
rticle Link (NCBI)
- ADDING SINGLE-DOSE DEXAMETHASONE TO ACUTE
MIGRAINE TREATMENT LOWERS RECURRENCE RATE
Summary This meta-analysis found that adding a single
dose of dexamethasone to standard abortive treatment for an acute
migraine lowers the risk that the migraine will recur within 72
hours.
Basis for Study/Article The authors explored the
role of parenteral dexamethasone in the treatment of acute migraine.
Detailed Summary of Study The authors analyzed the
data from seven randomized controlled trials comparing the effects
of standard abortive therapy for acute migraines plus either
parenteral dexamethasone or placebo.
Results/Body Adding dexamethasone to the regimen did
not improve pain relief, but it did reduce the risk of recurrence
within 72 hours (relative risk 0.74) compared to placebo.
Sources & Other Links
<> Colman I, et al. Parenteral dexamethasone for acute severe
migraine headache: meta-analysis of randomised controlled trials for
preventing recurrence. BMJ. 2008
Jun 14;336(7657):1359-61.
Article Link (NCBI)
- VITAMIN D
DEFICIENCY IS COMMON IN HEALTHY YOUNG CHILDREN
Summary Vitamin D deficiency (20 mg/mL) is common in
otherwise healthy young children, and a third of the children with
vitamin D deficiency had evidence of bone demineralization.
Significant predictors of deficiency were breastfeeding without
supplementation in infants and lower milk intake in children.
Basis for Study/Article The authors assessed the
prevalence of vitamin D deficiency in healthy infants and toddlers
and identified predictors of deficiency.
Detailed Summary of Study 25-hydroxyvitamin D levels
were measured in 380 healthy infants and toddlers at one urban
clinic. Information was also collected on the children’s sun
exposure, nutrition, and skin pigmentation and the parents’ health
habits. Deficiency was defined as a level 20 mg/mL; the “accepted
optimal threshold” was 30 mg/mL. For those found to have a
deficiency, wrist and knee x-rays were taken to assess bone
mineralization.
Results/Body 12% of the children had a vitamin D
deficiency; 40% had less than the optimal level. A third of the
children with deficiency had radiographic evidence of bone
demineralization and 7.5% had rachitic changes. In infants,
breastfeeding without supplementation was a significant predictor of
deficiency; in children, lower milk intake was a significant
predictor. Skin pigmentation was not a predictor.
Sources & Other Links Gordon CM, et al. Prevalence
of vitamin D deficiency among healthy infants and toddlers.
Arch Pediatr Adolesc Med. 2008
Jun;162(6):505-12.
Article Link (NCBI)
- CHILDREN
WHO DRINK 100% FRUIT JUICE HAVE BETTER NUTRIENT INTAKE AND AREN'T
OVERWEIGHT
Summary Children age 2 to 11 who drink 100% fruit juice
have better nutrient intake and are not more likely to be
overweight.
Basis for Study/Article The authors explored the
impact of consumption of 100% fruit juice in terms of dietary intake
and weight in children age 2 to 11 years.
Detailed Summary of Study The authors used data from
the 1999-2002 National Health and Nutrition Examination Survey (n =
3,618 children). Mean daily intake of 100% fruit juice was 4.1 fluid
ounces.
Results/Body Compared to those who didn’t drink 100%
fruit juice, the children who did drink 100% fruit juice had
significantly higher intakes of whole fruit, energy, carbohydrates,
vitamin C, vitamin B6, potassium, riboflavin, magnesium, iron and
folate. They had significantly less intake of total fat, saturated
fatty acids, discretionary fat and added sugar. The amount of juice
consumed did not affect the child’s weight or risk of being
overweight.
Sources & Other Links Nicklas T, et al. Association
between 100% juice consumption and nutrient intake and weight of
children aged 2 to 11 years. Arch Pediatr
Adolesc Med. 2008 Jun;162(6):557-65.
Article Link (NCBI)
- FDA RECALL
FOR IMMEDIATE RELEASE -- Pompano Beach, FL – July 01, 2008 –
Jack Distribution, LLC, 1501 Green Road Unit C Pompano Beach,
Florida 33064 and its wholesale distributors G & N works, Inc., and
Devine Distribution, Inc., announced today that they are conducting
a voluntary nationwide recall of the following lot numbers of the
company's supplement products sold under the brand names Rize 2
The Occasion and Rose 4 Her. (Rize 2 lot numbers CG-84
expires 11/10, GD-98 expires 08/10, CC-06 expires 06/10, 709 expires
09/10, CG-79 expires 11/10) (Rose 4 Her lot number CG-78 expires
11/10).
Jack Distribution, LLC, is conducting this recall after being
informed by representatives of the Food and Drug Administration
(FDA) that lab analysis by FDA of Rize 2 and Rose 4 Her samples from
lots manufactured and packaged in 2007 found the product contains
potentially harmful, undeclared ingredients. FDA asserts that its
chemical analysis revealed that these lots of Rize 2 The Occasion
and Rose 4 Her contain thiomethisosildenafil, an analog of
sildenafil, the active ingredient of a FDA-approved drug used for
Erectile Dysfunction (ED). FDA maintains that this ingredient is
close in structure to sildenafil and is expected to possess a
similar pharmacological and adverse event profile. This undeclared
chemical poses a potential threat to consumers because it may
interact with nitrates found in some prescription drugs (such as
nitroglycerin) and may lower blood pressure to dangerous levels.
Consumers with diabetes, high blood pressure, high cholesterol,
or heart disease often take nitrates. ED is a common problem in men
with these conditions, and consumers may seek these types of
products to enhance sexual performance.
Customers who have this product in their possession should stop
using it immediately and contact their physician if they have
experienced any problems that may be related to taking this product.
Any adverse events that may be related to the use of this product
should be reported to the FDA's MedWatch Program by phone at
1-800-FDA-1088 or by fax at 1-800-FDA-0178 or by mail at MedWatch,
HF-2, FDA, 5600 Fishers Lane, Rockville, MD 20852-9787.
The company advises that any unused portions from these lot
numbers be returned to the place of purchase for a full refund of
purchase price. G & N Works and Devine Distribution are not shipping
any Rize 2 or Rose 4 Her that is in stock while additional samples
are being tested, they expect to begin shipping again in 2-4 weeks.
Rize 2 and Rose 4 Her are sold in adult stores, vitamin &
nutrition shops, convenience stores, and via the internet
nationwide. The Rize 2 product is sold as a (single blister pack,
three count bottles, twelve count bottles, and thirty count bottles.
Rose 4 Her is only available in single blister packs and three count
bottles.
The Company is taking this voluntary action because it is
committed and is always concerned with the health of persons who
have consumed this product. The Company is reviewing the procedures
and policies of all firms involved with the manufacture of the
product to ensure that there will be no future issues with regard to
Rize 2 and Rose 4 Her pills composition. The Company is working
closely with the FDA in the recall process and is committed to the
quality and integrity of its products. It sincerely regrets any
inconvenience to consumers and its other customers.
FDA notified healthcare professionals that a BOXED WARNING and
Medication Guide are to be added to the prescribing information to
strengthen existing warnings about the increased risk of developing
tendinitis and tendon rupture in patients taking fluoroquinolones
for systemic use.
FOR IMMEDIATE RELEASE
Fluoroquinolones are associated with an increased risk of tendinitis
and tendon rupture. This risk is further increased in those over age
60, in kidney, heart, and lung transplant recipients, and with use
of concomitant steroid therapy. Physicians should advise patients,
at the first sign of tendon pain, swelling, or inflammation, to stop
taking the fluoroquinolone, to avoid exercise and use of the
affected area, and to promptly contact their doctor about changing
to a non-fluoroquinolone antimicrobial drug. Selection of a
fluoroquinolone for the treatment or prevention of an infection
should be limited to those conditions that are proven or strongly
suspected to be caused by bacteria
-
ALZHEIMER'S DISEASE IS NOW THE 6th
LEADING CAUSE OF DEATH
Preliminary death
statistics for 2006, released by CDC’s National Center for Health
Statistics in early June 2008, found that Alzheimer’s Disease
surpassed diabetes as the 6th leading cause of death in
the United States. To view the
press release, please visit:
http://www.cdc.gov/media/pressrel/2008/r080611.htm.
-
TRAUMATIC BRAIN INJURIES
AMONG OLDER AMERICANS CAN RESULT FROM FALLS
Traumatic brain injuries due to falls caused nearly 8,000 deaths and
56,000 hospitalizations in 2005 among Americans 65 and older,
according to a new report from the Centers for Disease Control and
Prevention released in the June issue of the Journal of Safety
Research. To learn more, please visit:
http://www.cdc.gov/ncipc/tbi/elder_fall.htm.
- CAR CRASHES
MORE COMMON IN
PATIENTS WITH
OBSTRUCTIVE SLEEP APNEA
Summary
Car accidents are more common in patients with obstructive sleep
apnea/hypopnea, and they are also more likely to be injured in the
crash.
Basis for Study/Article The authors of this Canadian
study investigated the incidence and severity of car accidents in
patients with obstructive sleep apnea.
Detailed Summary of Study Information on the number
and severity of vehicle accidents was obtained from 783 patients
(71% men, mean age 50 years) undergoing sleep studies for suspected
obstructive sleep apnea. The figures were compared to those from 783
age- and sex-matched controls.
Results/Body Over a 3-year period the patients had
252 car crashes and the controls had 123. Relative risks were 2.6
for patients with mild OSA, 1.9 for those with moderate OSA and 2.0
for those with severe OSA. The crashes involving OSA patients were
more likely to cause personal injury; corresponding relative risks
were 4.8, 3.0 and 4.3. The patients whose sleep studies were
negative did not have a significantly increased risk of being in a
crash compared to the controls, nor were they more likely to be
involved in accidents involving injury. 80% of the serious crashes
(head-on collisions or accidents involving pedestrians or cyclists)
occurred in the patients.
Commentary This data indeed is concerning for not
only the frequency of accidents, but the evidence that major lapses
in attention must have occurred to result in the higher severity of
each accident. Doctors of OSA patients need to counsel their
patients that this is a risk of OSA and consider this when
recommending therapy for OSA.
Grant E. Fraser, M.D.
MedAlert Editor
Sources & Other Links Mulgrew AT, et al. Risk and
severity of motor vehicle crashes in patients with obstructive sleep
apnoea/hypopnoea. Thorax. 2008
Jun;63(6):536-41.
Article
Link (NCBI)
-
LONG-TERM
EFFECTS OF DIET AND
EXERCISE ON TYPE 2
DIABETES
PREVENTION
Summary This
study from China found that lifestyle changes (diet and exercise)
can prevent or delay the onset of type 2 diabetes, but their effect
on reducing the risk of cardiovascular disease and death remains
unclear.
Basis for Study/Article The authors performed a
follow-up analysis of their diabetes prevention study to assess the
long-term effects of lifestyle changes. In the original multicenter
study (1986–1992), 577 adults with impaired glucose tolerance were
randomized to a control group or to one of three “lifestyle
intervention groups” (diet, exercise, or both).
Detailed Summary of Study In this follow-up study,
type 2 diabetes incidence, CVD incidence and mortality, and
all-cause mortality were tracked in the original trial participants.
Results/Body At the 20-year follow-up, 80% of those
who made lifestyle changes had developed type 2 diabetes vs. 93% of
the control group. Those who made lifestyle changes had a 51% lower
incidence of diabetes during the 6-year study and a 43% lower
incidence at the 20-year follow-up, “controlled for age and
clustering by clinic.” Average yearly incidence of diabetes was 7%
for those who made lifestyle changes vs. 11% in the control group.
Those who made lifestyle changes “spent an average of 3.6 fewer
years with diabetes” vs. the control group. There were no
differences between the groups in terms of rate of first CVD events,
CVD mortality, and all-cause mortality, “but our study had limited
statistical power to detect differences for these outcomes.”
Sources & Other Links Li G, et al. The long-term
effect of lifestyle interventions to prevent diabetes in the China
Da Qing Diabetes Prevention Study: a 20-year follow-up study.
Lancet 2008 May
24;371(9626):1783-9.Article
Link (NCBI)
- TEENS
WITH PRIMARY AMENORRHEA
AND PCOS
ARE A
DISTINCT SUBGROUP
Summary
Teenage girls with polycystic ovarian syndrome that manifests as
primary amenorrhea form a subgroup distinct from those with PCOS and
oligomenorrhea or secondary amenorrhea. They have “increased
features of the metabolic syndrome and higher androstenedione levels
and may represent a more severe spectrum of a common condition.”
Basis for Study/Article This study compared the
characteristics of teenage girls with PCOS manifested by primary
amenorrhea vs. that manifested by secondary amenorrhea or
oligomenorrhea.
Detailed Summary of Study At a Canadian pediatric
endocrine clinic, clinical, laboratory and ultrasound results were
collected from 9 adolescent girls with PCOS and primary amenorrhea
and 18 with PCOS and secondary amenorrhea or oligomenorrhea.
Results/Body The girls with primary amenorrhea and
PCOS had “older age at pubarche, higher androstenedione levels,
greater prevalence of family history of obesity, a tendency toward
no withdrawal bleeding in response to the progesterone challenge,
and more features associated with the metabolic syndrome.”
Sources & Other Links Rachmiel M, et al. Primary
amenorrhea as a manifestation of polycystic ovarian syndrome in
adolescents: a unique subgroup? Arch
Pediatr Adolesc Med. 2008 Jun;162(6):521-5.
Article Link (NCBI)
- MEN
WITH LOWER
VITAMIN D LEVELS HAVE A
HIGHER RISK OF
MYOCARDIAL INFARCTION
Summary
This prospective study found that men with lower levels of vitamin D
have a higher risk of myocardial infarction, with the degree of risk
dependent on the level.
Basis for Study/Article The authors investigated
whether low vitamin D levels raise the risk of coronary heart
disease in men.
Detailed Summary of Study As part of the Health
Professionals Follow-up Study, serum vitamin D levels
(25-hydroxyvitamin D) were measured at baseline in 18,225 men age 40
to 75 who did not have cardiovascular disease. 10 years later, 454
of the men had developed nonfatal MI or fatal CHD. The authors
compared vitamin D levels in those who did and did not develop heart
disease.
Results/Body The risk of having an MI was 2.42 times
higher in the men with low vitamin D levels (defined as
15 ng/mL), 1.43
times higher in those with levels 15 to 22.5 ng/mL, and 1.60 times
higher in those with levels 22.6 to 29.9 ng/mL vs. those with
“sufficient” levels (30
ng/mL). Adjusting for CV risk factors such as family history of MI,
BMI, alcohol consumption, physical activity, lipid profile and
others did not change the relationship.
Sources & Other Links Giovannucci E, et al.
25-hydroxyvitamin D and risk of myocardial infarction in men: a
prospective study. Arch Intern Med.
2008 Jun 9;168(11):1174-80.
Article Link (NCBI)
-
IN YOUNG ADULTS,
IBD HAS SERIOUS EFFECTS ON
QUALITY OF LIFE, BODY
IMAGE,
AND SEXUAL FUNCTION
Summary In young adults, IBD has serious effects on
quality of life, body image, and sexual function. “These issues need
to be further addressed in both research & clinical settings.”
Basis for Study/Article The authors of this study
from Australia explored how IBD affects quality of life, body image
and sexual function in young adults.
Detailed Summary of Study The authors asked 183
patients (65% women, mean age 36 years) how IBD (mostly Crohn’s
disease and ulcerative colitis) affected their lifestyle and body
image.
Results/Body 88% of the patients believed that IBD
had affected their quality of life. 52% believed it had affected
their relationship status; women were more likely to believe this,
even though there was no actual difference in relationship status
between men and women. 75% of women and half of men said it had
affected their body image. 67% of women and 39% of men reported
decreased libido due to IBD; 69% of those who had undergone surgery
reported decreased libido vs. 49% of those who had not. 55% of
patients reported decreased sexual activity since the onset of IBD
symptoms: 87% attributed the decrease to feeling unwell, 48% to
lower libido and 23% to concerns about their partner’s reaction.
Sources & Other Links Muller KR, et al. Female
gender and surgery lead to greater perceived impact of inflammatory
bowel disease (IBD) on body image and sexual function: a neglected
issue. Presented at Digestive Disease Week, May 2008, abstract #944
Article Link
(DOWNLOAD)
-
GREEN TEA MAY IMPROVE HEART FUNCTION
ACCORDING TO ONE NEW STUDY-MORE STUDIES NEEDED TO CONFIRM
More evidence for the beneficial effect of green tea on risk factors
for heart disease has emerged in a new study reported in the latest
issue of European Journal of Cardiovascular Prevention and
Rehabilitation. The study found that the consumption of green tea
rapidly improves the function of (endothelial) cells lining the
circulatory system; endothelial dysfunction is a key event in the
progression of atherosclerosis.
The study, performed by Dr Nikolaos Alexopoulos and colleagues at
the 1st Cardiology Department, Athens Medical School in Greece, was
a randomized trial involving the diameter measurement (dilatation)
of the brachial artery of healthy volunteers on three separate
occasions - after taking green tea, caffeine, and hot water (for a
placebo effect). The measurements were taken at 30, 90 and 120
minutes after consumption. Dilatation of the brachial artery as a
result of increased blood flow (following a brief period of ischemia
of the upper limb) is related to endothelial function and is known
to be an independent predictor of cardiovascular risk.2
Results showed that endothelium-dependent brachial artery
dilatation increased significantly after drinking green tea, with a
peak increase of 3.9 per cent 30 minutes after consumption. The
effect of caffeine consumption (or hot water) was not significant.
While black tea has been associated with improved short and
long-term endothelial performance, this is the first time that green
tea has been shown to have a short-term beneficial effect on the
large arteries. Another study has already shown that green tea
reverses endothelial dysfunction in smokers.
Green tea, which originates in China but is now consumed
throughout the world, is made with pure leaves, and has undergone
little oxidization during processing. The cardiovascular benefits of
all teas - as well as dark chocolate and red wine - are attributed
to the flavonoids they contain and their antioxidant activity.3
However, says investigator Dr. Charalambos Vlachopoulos, flavonoids
in green tea are probably more potent antioxidants than in black tea
because there has been no oxidization.
"These findings have important clinical implications," says Dr
Vlachopoulos. "Tea consumption has been associated with reduced
cardiovascular morbidity and mortality in several studies. Green tea
is consumed less in the Western world than black tea, but it could
be more beneficial because of the way it seems to improve
endothelial function. In this same context, recent studies have also
shown potent anticarcinogenic effects of green tea, attributed to
its antioxidant properties."
- ICY HOT HEAT THERAPY AIR
ACTIVATED HEAT FOR BACK, ARM, NECK AND LEG RECALLED
What is “Icy Hot Heat Therapy Air Activated Heat”?
Icy Hot Heat Therapy Air Activated Heat
is an adhesive patch that generates heat. The patch comes in
a red sealed plastic pouch. Once the pouch is opened and the
patch is exposed to air, the chemicals contained in the patch
activate to produce heat. It is then applied to body surfaces to
relieve muscle and joint pain associated with arthritis,
backache, muscle strains and sprains.
What is the problem with Icy Hot Heat Therapy Air
Activated Heat products?
Chattem, Inc. chose to recall their Icy Hot Heat Therapy
products because they received consumer reports of first, second
and third degree burns as well as skin irritation and skin
removal resulting from the use of the Icy Hot Heat Therapy Air
Activated Heat patch. As part of FDA's recall classification
process, we will be reviewing the firm's root-cause analysis on
what caused the burns.
What is the difference between first, second and
third degree burns?
The type of burn is determined by how deeply it penetrates
into the skin. There are two main layers of skin, and the degree
of burn is based on how each layer is affected. First degree
burns are the least severe and third degree burns are the
deepest or most severe.
First Degree Burns: Means the top layer of skin (the
epidermis) is damaged but not destroyed and turns bright pink or
very red. Pain from first degree burns ranges from mild to
extreme. No skin comes off and there are no blisters. Mild
sunburns are a good example of first degree burns.
Second Degree Burns: Means burn damage has gone
through the top layer (the epidermis) and into the 2nd layer of
skin (the dermis). The top layer of skin is destroyed and may
slide off or blister. Blisters are the first sign of a second
degree burn. The wound appears red or pink and moist. Second
degree burns are the most painful kind of burn.
Third Degree Burns: Means the burn has destroyed
both the first and second (epidermis and dermis) layers of the
skin. The exposed wound appears white, gray, yellow, brown or
black and is usually dry. There may be little or no pain or the
area may feel numb because of nerve damage.
When were the Icy Hot Heat Therapy Air Activated
Heat patches produced and sold?
The firm issued a press release, dated February 8, 2008, for
their voluntary recall involving 2.3 million Icy Hot Heat
Therapy Air Activated Heat patches distributed in the United
State since December 2006. The products were manufactured
between December 2006 and February 2008 and sold over the
counter through food, drug and mass merchandisers. You can find
a listing of retailers on Chattem, Inc.’s website at
http://www.chattem.com/wheretobuy/icy.asp.
What products are affected by the recall?
All lots and all sizes of the following Icy Hot Heat Therapy
products are affected by this recall:
- Icy Hot Heat Therapy Air Activated Heat - Back
- Icy Hot Heat Therapy Air Activated Heat - Arm, Neck, and
Leg
- Icy Hot Heat Therapy Air Activated Heat - Arm, Neck, and
Leg in single-use “samples” that were included on a limited
promotional basis in yellow and red cartons of 3
oz. Aspercreme Pain Relieving Crčme.
The samples were distinct and stand-alone products, clearly
labeled as "Icy Hot Heat Therapy Air Activated Heat."
This recall only involves the above listed Icy Hot
Heat Therapy products and does not involve any other Icy Hot
products such as the medicated patch, cream, or balm/stick
that also use the “Icy Hot” name. -Author FDA
- HIGH FIBER DIET
IMPROVED CONSTIPATION IN WOMEN WITH PELVIC FLOOR DISORDERS AKA THE
BULK OF THE STUDY
Constipation is a common and potentially burdensome problem,
particularly among women with pelvic floor disorders.
Nonpharmacologic treatment usually should be the first step. In a
study evaluating whether augmenting dietary fiber can lessen
self-reported constipation severity and laxative use, investigators
recruited 41 women (mean age, 60) with constipation and a history of
pelvic floor disorders. Twenty-five women had had previous surgery
for pelvic organ prolapse. Participants were supplied with and
instructed to eat high-fiber cereal, starting with one-quarter cup
(7 g fiber) daily and gradually increasing to 1 cup per day (28 g
fiber) during the 42-day study period. Women also were instructed to
increase water intake and decrease caffeine consumption. In addition
to maintaining daily diaries, women reported their constipation
symptoms in standardized telephone interviews every 2 weeks.
Six women withdrew from the study because they could not tolerate
the high-fiber diet. Thirty women completed the study and reported
less straining, less frequent sensations of incomplete emptying, and
less frequent vaginal or perineal splinting than at baseline. Based
on the Patient Assessment of Constipation Symptoms scale,
participants reported improved abdominal, rectal, and stool
symptoms. Caffeine intake decreased significantly, water intake
remained largely unchanged, and weekly laxative use decreased by
about half during follow-up.
Comment: This simple prospective study demonstrates
that increased fiber intake can help relieve constipation,
particularly in women with pelvic floor disorders. The lack of a
control group makes it difficult to compare this approach to others,
and the multifaceted intervention makes it difficult to assess
whether increased fiber consumption was the only factor that
improved symptoms. Regardless, because low fiber intake often
contributes to constipation, this treatment approach merits
consideration by clinicians for their patients who are amenable to
fiber supplementation. Cereal brands with the word "fiber" on the
box are a good starting point; but because of the considerable
confusion about high-fiber cereals, encouraging patients to read the
rest of the nutritional information on the box is important.
—
Sandra Ann Carson, MD
RISEDRONATE (Actonel®)
PREVENTS BONE LOSS IN IBD
PATIENTS ON STEROIDS
Summary This randomized controlled trial found that
risedronate (Actonel®) prevents steroid-induced bone loss in IBD.
Basis for Study/Article The authors of this study
from England examined the efficacy of risedronate for preventing
steroid-related bone loss in patients with IBD.
June 25, 2008
Detailed Summary of Study Patients receiving
prednisolone for an IBD flare-up were randomized to receive placebo
or risedronate, in addition to calcium and vitamin D. DEXA scans of
the lumbar spine and hips were done at baseline and 8 weeks later in
73 patients (42 with ulcerative colitis, 31 with Crohn’s disease;
average age 43.5 years; 42 patients were men).
Results/Body In the lumbar spine, the patients
taking risedronate had a 1% gain in BMD vs. no change in the placebo
group after 2 months of treatment. In the total hip, neither group
experienced BMD change. In Ward’s triangle (neck of the femur), the
risedronate group had a 1% loss and the placebo group had a 2% loss.
Sources & Other Links Kriel MH, et al. Risedronate
protects against bone loss when a relapse of IBD is treated with
steroids. Abstract #T1122 presented at Digestive Diseases Week, May
2008.
Article Link (DOWNLOAD)
IM
DEXAMETHASONE +
ANTIBIOTICS USEFUL FOR
ACUTE
EXUDATIVE PHARYNGITIS
Summary This randomized controlled trial found that for
acute exudative pharyngitis, adding a single dose of IM
dexamethasone to the antibiotic regimen relieves symptoms better
than antibiotics alone.
June 25, 2008
Basis for Study/Article The authors of this
single-center trial from Turkey tested the efficacy of a single dose
of IM dexamethasone in the treatment of acute exudative pharyngitis.
Detailed Summary of Study Adults with acute
exudative pharyngitis, sore throat, and/or odynophagia were
randomized to receive either an 8-mg IM dose of dexamethasone (n =
31) or placebo (n = 42), in addition to 3 days of azithromycin and
paracetamol (acetaminophen). Time to onset of pain relief and time
to complete pain relief were compared.
Results/Body Onset of pain relief occurred in 8.06
hours in the dexamethasone group vs. 19.90 hours in the placebo
group. Corresponding figures for complete pain relief were 28.97
hours and 53.74 hours.
Sources & Other Links Tasar A, et al. Clinical
efficacy of dexamethasone for acute exudative pharyngitis.
J Emerg Med. 2008 May 10. [Epub
ahead of print]
Article Link (NCBI)
-
TIGHT DIABETES
CONTROL LOWERS
INCIDENCE OF NEPHROPATHY,
VASCULAR EVENTSSummary This large study with 5
years of follow-up found that tight diabetes control (using
gliclazide [Diamicron®] and other drugs to obtain an HbA1c of 6.5%
or less) lowers the incidence of macrovascular and microvascular
events together, in particular reducing the relative risk of
nephropathy by 21%.
Basis for Study/Article The ADVANCE Collaborative
Group tested the effects of intensive glucose control on
macrovascular and microvascular outcomes in patients with type 2
diabetes.
June 25, 2008
Detailed Summary of Study 11,140 patients with type
2 diabetes were randomized to receive either standard glucose
control or intensive control (using modified-release gliclazide [Diamicron®]
and other drugs to obtain an HbA1c of 6.5% or less). After a median
follow-up of 5 years, the number of major macrovascular events (CV
death, nonfatal MI, nonfatal stroke) and major microvascular events
(nephropathy, retinopathy) was assessed.
Results/Body At follow-up, mean HbA1c levels were
6.5% in the intensive group vs. 7.3% in the standard group. Combined
major and minor macrovascular events occurred in 18.1% of the
intensive group vs. 20% of the standard group (p = 0.01). Major
microvascular events occurred in 9.4% of the intensive group vs.
10.9% of the standard group (p = 0.01). Nephropathy occurred in 4.1%
of the intensive group vs. 5.2% of the standard group. There were no
differences between the groups in the incidence of major
macrovascular events alone, retinopathy, CV death or all-cause
mortality. Severe hypoglycemia occurred in 2.7% of the intensive
group vs. 1.5% of the standard group (p <0.001).
Sources & Other Links ADVANCE Collaborative Group.
Intensive blood glucose control and vascular outcomes in patients
with type 2 diabetes. N Engl J Med.
2008 Jun 12;358(24):2560-2572.
Article Link (NCBI)
-
SEQUENTIAL THERAPY IS BETTER THAN STANDARD TRIPLE
THERAPY FOR H. PYLORI
Summary This meta-analysis
found that 10-day sequential therapy is better than standard triple
therapy for the treatment of H. pylori
infection in treatment-naďve patients. However, the authors caution
that most of the patients in the studies they reviewed were from
Italy, only one study was double-blinded, and publication bias may
have played a role.
June 25, 2008
Basis for Study/Article Because standard triple
therapy for H. pylori infection
is unsuccessful in about a quarter of patients, the authors
conducted a meta-analysis on the efficacy of sequential therapy in
treatment-naďve patients.
Detailed Summary of Study The reviewers analyzed
data from 10 randomized controlled trials (n = 2,747) comparing
sequential vs. standard therapy.
Results/Body H. pylori
eradication rates were 93.4% in the 1,363 patients receiving
sequential therapy and 76.9% in the 1,384 patients receiving
standard triple therapy. The success rate was affected by the
patient’s smoking status, diagnosis and method of diagnosis,
resistance to clarithromycin or imidazoles, and duration of triple
therapy. Adherence rates were 97.4% for sequential therapy and 96.8%
for standard therapy. Adverse effects were similar. The authors
believe that if trials in other countries confirm the findings,
“10-day sequential therapy could become a standard treatment for
H. pylori infection in
treatment-naďve patients.”
Commentary What is sequential therapy? Triple
therapy has been common for some time. One article detailing one
sequential regimen is available at:
http://www.annals.org/cgi/content/abstract/146/8/556
Briefly; the protocol used was:
| • |
|
Days 1-5
| › |
|
40 mg pantoprazole BID |
| › |
|
1 gram amoxicillin BID |
|
| • |
|
Days 6-10
| › |
|
40 mg pantoprazole BID |
| › |
|
500 mg clarithromycin BID |
| › |
|
500 mg tinidazole BID |
|
Grant E. Fraser, M.D. MedAlert Editor
Sources & Other Links Jafri NS, et al.
Meta-analysis: Sequential therapy appears superior to standard
therapy for Helicobacter pylori
infection in patients naive to treatment.
Ann Intern Med. 2008 May 19. [Epub ahead of print]
Article Link (NCBI)
- DEPRESSION AND TOO MUCH OR TOO LITTLE
ACTIVITY CAN LEAD TO PERSISTENT ADOLESCENT FATIGUE
Summary Teenagers
with depressive symptoms and either sedentary or highly active lives
are at risk for persistent fatigue.
June 18, 2008
Basis for Study/Article The authors of this British study
identified risk factors for persistent adolescent fatigue, defined
as extreme tiredness twice weekly or more often in the previous
month.
Detailed Summary of Study 1,880 subjects age 11 to 16 (49%
boys, 81% nonwhite) at 28 London schools completed questionnaires in
2001 and 2003 asking about persistent fatigue, activity level,
depressive symptoms, BMI and smoking status.
Results/Body 4% (84 students) of the students
reported persistent fatigue; however, in both surveys (2001 and
2003) only 3 students reported chronic fatigue syndrome. Persistent
fatigue was more common in teens who had depressive symptoms (odds
ratio 2.0), who were sedentary more than 4 hours a day (odds ratio
1.6) or who were extremely active (odds ratio 1.5). BMI and smoking
were not factors. Severe fatigue occurred in 11% of students aged 11
to 14 years and 17% of those aged 13 to 16 years.
Sources & Other Links Viner RM, et al. Longitudinal
risk factors for persistent fatigue in adolescents.
Arch Pediatr Adolesc Med. 2008
May;162(5):469-75.
Article Link (NCBI)
-
TABLE FOR CHRONIC ANTIHYPERTENSIVE DRUGS FROM THE USFDA - 2008
| Pharmacologic Class
|
Approved Drugs |
| aldosterone antagonists
Works on the blood side of the
nephron-binds to aldosterone. |
eplerenone, spironolactone |
| alpha adrenergic blockers |
doxazosin,
phenoxybenzamine, phentolamine, prazosin,
terazosin |
| angiotensin converting enzyme
inhibitors |
benazepril, captopril,
enalapril, fosinopril, lisinopril,
moexipril, perindopril, quinapril, ramipril,
trandolapril |
| angiotensin II receptor
blockers |
candesartan,
eprosartan, irbesartan, losartan,
olmesartan, telmisartan, valsartan |
| arteriolar vasodilators |
hydralazine, minoxidil |
| autonomic ganglionic
vasodilators |
mecamylamine |
| beta adrenergic blockers |
acebutolol,
atenolol, betaxolol, bisoprolol,
carvedilol, carteolol, esmolol, labetolol,
metoprolol, nadolol, penbuterol,
pindolol,
propranolol, timolol |
| catecholamine-depleting
sympatholytics |
deserpidine, reserpine |
| central alpha-2 adrenergic
agonists |
clonidine,
guanabenz, guanfacine, methyldopa |
| calcium channel blockers |
diltiazem,
verapamil |
| dihydropyridine calcium channel
blockers |
amlodipine,
felodipine, isradipine,
nicardipine, nifedipine,
nisoldipine |
| loop diuretics |
bumetanide, ethacrynic acid,
furosemide, torsemide |
| potassium-sparing diuretics |
amiloride,
triamterene |
| renin inhibitors |
aliskiren |
| thiazide diuretics
↓
Left
ventricular hypertropy. |
chlorothiazide, hydrochlorothiazide, hydroflumethiazide,
methyclothiazide, polythiazide |
| thiazide-like diuretics |
chlorthalidone,
indapamide, metolazone |
-
BLACK BOX
WARNING FROM FDA
June 16, 2008
FDA notified healthcare professionals that both conventional and
atypical antipsychotics are associated with an increased risk of
mortality in elderly patients treated for dementia-related
psychosis. In April 2005, FDA notified healthcare professionals that
patients with dementia-related psychosis treated with atypical
antipsychotic drugs are at an increased risk of death. Since issuing
that notification, FDA has reviewed additional information that
indicates the risk is also associated with conventional
antipsychotics. Antipsychotics are not indicated for the treatment
of dementia-related psychosis. The prescribing information for all
antipsychotic drugs will now include the same information about this
risk in a BOXED WARNING and the WARNINGS section.
- FALLS AND FALL-RELATED INJURIES AMONG PERSONS
AGED 65 YEARS OLD OR GREATER
- HAVING 1/2 TO 1 ALCOHOLIC DRINK PER DAY
PROTECTS AGAINST HIP FRACTURE
Summary
This meta-analysis found that people who have 1/2 to 1 alcoholic
drink per day have a lower risk of hip fracture compared to
nondrinkers and heavier drinkers.
Basis for
Study/Article
The authors performed a literature review to assess the effects of
moderate alcohol consumption on bone density and the risk of
osteoporotic hip fracture.
June 11, 2008
Detailed
Summary of Study
Effect sizes were pooled for hip fracture and bone density, and
results were synthesized for four outcomes: non-hip fracture, bone
density loss over time, bone response to estrogen replacement, and
bone remodeling.
Results/Body
People who had 1/2 to 1 alcoholic drink per day had a lower risk of
hip fracture compared to nondrinkers (relative risk 0.80); the
relative risk was 1.39 for those who had more than 2 drinks a day.
“A linear relationship existed between femoral neck bone density and
alcohol consumption,” but “a precise range of beneficial alcohol
consumption cannot be determined.”
Sources &
Other Links
Berg KM, et al. Association between alcohol consumption and both
osteoporotic fracture and bone density.
Am J Med. 2008
May;121(5):406-18.
Article Link (NCBI)
-
OBSTRUCTIVE SLEEP APNEA IS COMMON IN WOMEN WITH
NOCTURIA
Summary
Obstructive sleep apnea is common in women with nocturia, and 88% of
women with dilute nighttime urine have OSA. “We should consider a
diagnosis of OSA in all patients with nocturia,” even those with
daytime overactive bladder symptoms.
June 11, 2008
Basis for
Study/Article
The authors explored the association between obstructive sleep apnea
and nocturia in women and tested urine samples to see whether urine
concentration was predictive for sleep apnea.
Detailed
Summary of Study
21 women with nocturia (16 of them also had daytime overactive
bladder) and 10 control subjects completed nocturia questionnaires,
underwent a home sleep study and provided evening and morning urine
samples.
Results/Body
17 of the 21 women with nocturia (81%) were found to have sleep
apnea (13 of the 16 with daytime overactive bladder and 4 of the 5
without) vs. 4 of the control group. “The presence of diluted
nighttime urine in a patient with nocturia was 88% sensitive for the
presence of OSA.”
Sources &
Other Links
Lowenstein L, et al. The relationship between obstructive sleep
apnea, nocturia, and daytime overactive bladder syndrome in women.
Am J Obstet Gynecol. 2008
May;198(5):598.e1-5.
- VOLUNTARY RECALL OF SINGLE LOT MORPHINE
ETHEX
Corporation notified healthcare professionals of a voluntary recall
of a single lot of morphine sulfate 60 mg extended release tablets
(Lot No. 91762) due to a report of a tablet with twice the
appropriate thickness. Oversized tablets may contain as much as two
times the labeled level of active morphine sulfate. The lot was
distributed by ETHEX Corporation under an "ETHEX" label between
April 16th and April 27th of 2008. Opioids such as morphine have
life-threatening consequences if overdosed. Consequences can include
respiratory depression (difficulty or lack of breathing), and low
blood pressure. Many patients for whom this product is prescribed
are likely to be highly debilitated with reduced strength or energy
as a result of illness, and may be less likely to determine that a
tablet is overweight or oversized than an unimpaired individual. If
consumers have any questions about the recall, they should call
their physician, pharmacist, or other health care provider.
- ADVERSE EVENTS ASSOCIATED WITH PCA AND
INSULIN PUMPS IN ADOLESCENTS
Summary
Over a 10-year period, there were 1,594 reports to the FDA of
adverse events associated with adolescents’ use of insulin pumps
(including 13 deaths) and 53 reports of adverse events associated
with patient-controlled analgesia pumps. “Studies need to further
identify safety problems in this age group.”
Basis for
Study/Article
After receiving five reports of deaths in adolescents associated
with insulin pumps in 2005, the FDA conducted an assessment of the
safety of insulin and PCA pumps in this population.
June 4, 2008Detailed
Summary of Study
The authors reviewed reports submitted to the FDA from 1996 through
2005 about adverse events associated with use of insulin or PCA
pumps by adolescents (ages 12 to 21). Demographics, type of adverse
event, outcomes and contributing factors were analyzed.
Results/Body
Over a 10-year period, there were 1,594 reports of adverse events
associated with insulin pumps, including 13 deaths, 2 possible
suicide attempts, and several reports of apparently device-related
hyperglycemia or hypoglycemia. Some of the contributing factors were
compliance problems, lack of education, “sports-related activities”
and “dropping or damaging the pump.” In 82% of the events the
patient was hospitalized. There were 53 reports of adverse events
associated with PCA pumps. In half the patients received too much
medication; “tampering and noncompliance were evident in some
cases.”
The authors
suggest more studies on the safety of these devices in adolescents.
Sources &
Other Links
Cope J, et al. Adolescent use of insulin and patient-controlled
analgesia pump technology: a 10-year Food and Drug Administration
retrospective study of adverse events. Pediatrics. 2008 May;121(5):e1133-8.
Article Link (NCBI)
-
DRUG RECALLS
LISTED:
Abbott
notified consumers and healthcare professionals of the recall of
two lots of Calcilo XD Low-Calcium/vitamin D-Free Infant Formula
with Iron powder, a low-calcium and Vitamin D-free infant
formula specifically designed for the nutrition support of
infants and children with hypercalcemia. The product,
distributed in the United States between 06/06/06 and 04/17/08,
is being recalled because small amounts of air may have entered
the can, resulting in product oxidation. Consumption of highly
oxidized foods can cause gastrointestinal symptoms such as
nausea, vomiting, and diarrhea. Parents should contact their
healthcare professional if they have any questions or concerns.
June 02, 2008
International Pharmaceuticals, Ltd. and FDA notified consumers
and healthcare professionals that the company is recalling all
supplement products sold under the brand name of Viril-ity Power
(VIP) Tablets. The product is being recalled because one lot was
found to contain a potentially harmful undeclared ingredient,
hydroxyhomosildenafil, an analog of sildenafil. Sildenafil is
the active ingredient in Viagra, an FDA-approved drug used for
erectile dysfunction. The undeclared ingredient may interact
with nitrates found in some prescription drugs (such as
Nitroglycerin) and may lower blood pressure to life-threatening
levels. Consumers with diabetes, high blood pressure, high
cholesterol, or heart disease often take such nitrates.
Consumers who have Viril-ity Power (VIP) Tablets should stop
using it immediately and contact their healthcare professional
if they experience any problems that may be related to taking
this product.
May 30,
2008
FDA
informed consumers not to use or purchase Mommy's Bliss Nipple
Cream, marketed by MOM Enterprises, Inc., because the product
contains potentially harmful ingredients that may cause
respiratory distress or vomiting and diarrhea in infants. The
product is promoted to nursing mothers to help soothe and heal
dry or cracked nipples. Potentially harmful ingredients in the
product are chlorphenesin and phenoxyethanol. Chlorphenesin
relaxes skeletal muscle and can depress the central nervous
system and cause slow or shallow breathing in infants.
Phenoxyenthanol, a preservative that is primarily used in
cosmetics and medications, can also depress the central nervous
system and may cause vomiting and diarrhea, which can lead to
dehydration in infants. Mothers and caregivers should seek
immediate medical attention if their child shows signs and
symptoms of decreases in appetite, difficulty in awakening,
limpness of extremities or a decrease in an infant's strength of
grip and a change in skin color.
May 29,
2008
FDA
alerted consumers and healthcare professionals not to buy or use
Xiadafil VIP Tablets sold in bottles of 8 tablets (Lot #6K029)
or blister cards of 2 tablets (Lot# 6K029-SEI). The product is
marketed as a dietary supplement and is promoted and sold over
the internet for sexual enhancement and to treat erectile
dysfunction (ED). The product contains a potentially harmful,
undeclared ingredient that may dangerously affect a person's
blood pressure and can cause other life-threatening side
effects. Xiadafil VIP Tablets contain hydroxyhomosildenafil, an
analog of sildenafil, the active ingredient in Viagra, an FDA
approved prescription drug for ED. The undeclared ingredient may
interact with nitrates found in some prescription drugs and can
lower blood pressure to life-threatening levels. Consumers with
diabetes, high blood pressure, high cholesterol, or heart
disease often take nitrates. Consumers who have used the product
should discontinue use immediately and consult their healthcare
professional if they have experienced any adverse events that
they believe may be related to the use of this product.
-
FDA AND CDC ISSUE
ALERT ON MENACTRA
MENlNGOCOCCAL
VACCINE AND GUILLAIN BARRE SYNDROME
The Food and Drug Administration (FDA) and Centers for
Disease Control and Prevention (CDC) are alerting consumers and
health care providers to five reports of Guillain Barre Syndrome
(GBS) following administration of Meningococcal Conjugate
Vaccine A, C, Y, and W135 (trade name Menactra), manufactured by
Sanofi Pasteur. It is not known yet whether these cases were
caused by the vaccine or are coincidental. FDA and CDC are
sharing this information with the public now and actively
investigating the situation because of its potentially serious
nature.
Guillain Barre Syndrome (GBS) is a serious neurological
disorder that can occur, often in healthy individuals, either
spontaneously or after certain infections. GBS typically causes
increasing weakness in the legs and arms that can be severe and
require hospitalization.
Meningococcal infection, which Menactra prevents, is a major
cause of bacterial meningitis, affecting approximately 1 in
100,000 people annually. The infection can be life threatening:
10-14 percent of cases are fatal and 11-19 percent of survivors
may have permanent disability.
According to Jesse Goodman, MD, Director of FDA’s Center for
Biologics Evaluation and Research, at the present time there are
no changes in recommendations for vaccination; individuals
should continue to follow their doctors' recommendations. FDA
and CDC are not able to determine if any or all of the cases
were due to vaccination. The current information is very
preliminary and the two agencies are continuing to evaluate the
situation.
Because of the potentially serious nature of this matter, FDA
and CDC are asking any persons with knowledge of any possible
cases of GBS occurring after Menactra to report them to the
Vaccine Adverse Event Reporting System (VAERS) to help the
agencies further evaluate the matter. Individuals can report to
VAERS on the web at www.vaers.hhs.gov <http://www.vaers.hhs.gov>
or by phone at 1-800-822-7967.
The five cases of GBS reported following administration of
Menactra occurred in individuals living in NY, OH, PA, and NJ.
All five patients were 17 or 18 years of age and developed
weakness or abnormal sensations in the arms or legs, two-four
weeks after vaccination. All individuals are reported to be
recovering or to have recovered. More than 2.5 million doses of
Menactra vaccine have been distributed to date. The rate of GBS
based on the number of cases reported following administration
of Menactra is similar to what might have been expected to occur
by coincidence, that is, even without vaccination. However, the
timing of the events is of concern. Also, vaccine adverse events
are not always reported to FDA so there may be additional cases
of which we are unaware at this time.
Prelicensure studies conducted by Sanofi Pasteur of more than
7000 recipients of Menactra showed no GBS cases. CDC conducted a
rapid study using available health care organization databases
and found that no cases of GBS have been reported to date among
110,000 Menactra recipients .
-
CONSUMER
ALERT
Some
say that the age of chivalry is past, that the spirit of romance is dead. The age of chivalry is never past, so long as there is a wrong
left unredressed on earth."
Charles Kingsley,
Vol., II, Ch 28:
"A
good conscience is a continual Christmas." Ben Franklin

Beat the Press News Exclusive:
The following resources have been compiled by
USCDC as a resource for older
adults, their families, friends or caregivers, and those who would
like to contribute to the relief efforts
following the devastation caused by
Hurricane Katrina along the US gulf coast.
The web pages of the following organizations that are principals in
disaster relief provide information on donating cash,
volunteers and products. Each organization
also states how they are aiding relief
efforts.
American Red Cross
http://www.redcross.org/
To donate: Call 1-800-HELP NOW or 1-800-257-7575 (Spanish).
Internet users can make a secure online
contribution by visiting
www.redcross.org.
To volunteer: Individuals interested in volunteering for the
American Red Cross should contact their
local Red Cross chapter.
America's Second Harvest
(non-governmental hunger-relief organization)
http://www.secondharvest.org/
To donate: Internet users can make a secure online contribution by
visiting
www.secondharvest.org.
Companies, manufacturers or retailers wanting to donate a full
truckload of dry storage product, call
1-800-771-2303 and ask for the Food
Sourcing Department Companies wanting to donate transportation of
product, call 1-800-771-2303 and ask for the Logistics Department
The Humane Society of the United States
http://www.hsus.org/
To donate: Internet users can make a secure online contribution by
visiting www.hsus.org.
The American Geriatrics Society
Hurricane Katrina: Informational Resources
http://www.americangeriatrics.org/news/hurricane_katrina.shtml
Comprehensive list of sources of medical information for clinicians
and caregivers, plus disaster and relief
information.
Federal Emergency Management Agency (FEMA)
http://www.fema.gov/
The US federal agency in charge of disaster regularly updates
information on relief efforts, and provides links to a number
of disaster relief organizations.
Hospice Foundation of America Establishes Hospice Patient Locater
Message Board at
www.hospicefoundation.org in Response to Hurricane Katrina
The Salvation Army is currently providing services to storm
survivors and first responders in the Gulf
Coast states as well. You can visit their
website at
www.salvationarmy.com
God Bless the US CDC and the United States of
America.-"InfoJustice"
-
FDA's New Influenza Vaccine for
Upcoming Flu Season
The Food and Drug Administration (FDA) today approved Fluarix, an
influenza vaccine for adults that contains inactivated virus.
Fluarix is approved to immunize adults 18 years of age and older
against influenza virus types A and B contained in the vaccine.
Influenza is also commonly called the flu.
"FDA"s approval of Fluarix is a big step toward providing an
adequate supply of flu vaccine for the American public," said Mike
Leavitt, Secretary of Health and Human Services (HHS). "Having more
manufacturers of influenza vaccine licensed in the U.S., and having
more vaccine dosages, is critical to public health and I applaud FDA
for taking such quick action to obtain and evaluate the data needed
to license Fluarix in time for this year"s influenza season."
The approval of Fluarix breaks new ground in that it is the first
vaccine approved using FDA"s accelerated approval process.
Accelerated approval allows products that treat serious or
life-threatening illnesses to be approved based on successfully
achieving an endpoint that is reasonably likely to predict ultimate
clinical benefit, usually one that can be studied more rapidly than
showing protection against disease. In this case, the manufacturer
demonstrated that after vaccination with Fluarix adults made levels
of protective antibodies in the blood that FDA believes are likely
to be effective in preventing flu. GlaxoSmithKline, the manufacturer
of Fluarix, will do further clinical studies as part of the
accelerated approval process to verify the clinical benefit of the
vaccine.
"Previous shortages highlighted the need for additional influenza
vaccine manufacturers for the U.S. market," said FDA Commissioner
Lester Crawford. "Accelerated approval has allowed us to evaluate
and approve Fluarix in record time so that we can make available
additional safe and effective flu vaccines. I commend our Center for
Biologics for taking extraordinary steps to help us be better
prepared for both the upcoming and future flu seasons."
This success required close cooperation among the FDA, the
National Institutes of Health, and the product manufacturer," said
Dr. Jesse Goodman, Director of FDA"s Center for Biologics Evaluation
and Research. "The dedicated staff of this Center is doing
everything possible to prepare for the upcoming flu season."
FDA based the accelerated approval of Fluarix on thorough
evaluation of safety and effectiveness data from four clinical
studies involving approximately 1,200 adults. Other data from
post-marketing reports in other countries where Fluarix is already
approved were also reviewed as part of FDA"s safety assessment.
In the United States it is estimated that more than 200,000
people are hospitalized from flu complications, and about 36,000
people die from flu each year. Although no vaccine is 100% effective
against preventing disease, vaccination is the best protection
against influenza and can prevent many illnesses and deaths.
Fluarix is manufactured in Dresden, Germany by Sächsisches
Serumwerk (SSW), a subsidiary of GlaxoSmithKline Biologicals, of
Rixensart, Belgium. It will be distributed by GSK in Research
Triangle Park, NC.
-
FDA STRENGTHENS RISK MANAGEMENT PROGRAM;
ISOTRETINOIN (ACCUTANE) DURING PREGNANCY
The U.S. Food and Drug Administration (FDA) is announcing
approval of a strengthened distribution program for isotretinoin,
called iPLEDGE, aimed at preventing use of the drug during
pregnancy. Women who are pregnant or who might become pregnant
should not take the drug. Isotretinoin (Accutane and its generics)
is a highly effective drug for severe recalcitrant nodular acne, but
it carries a significant risk of birth defects if taken during
pregnancy.
The manufacturers are implementing a program that requires
registration in iPLEDGE by doctors and patients who agree to accept
specific responsibilities before receiving authorization to
prescribe or use the drug. These measures are designed to guard
against pregnancies while using the drug. Wholesalers and pharmacies
must also comply with the manufacturers' program requirements in
order to distribute and dispense the product. FDA is approving this
program under its regulations, known as Subpart H, that require
restrictions on the distribution of a drug to assure safe use.
"This stronger program is a major step in protecting against
inadvertent pregnancy exposure by tightly linking negative pregnancy
testing with dispensing of isotretinoin." said Dr. Steven Galson,
Director, FDA's Center for Evaluation and Research. "iPLEDGE, using
a computer-based and telephone system, will provide health care
professionals with the real time information necessary to
effectively manage the risks of isotretinoin."
In February 2004, at a joint meeting, FDA's Drug Safety and Risk
Management Advisory Committee and Dermatologic and Ophthalmic Drugs
Advisory Committee reviewed the existing isotretinoin risk
management programs in effect at that time. Based upon their review,
the joint committee called for major improvements in the restricted
distribution program, including mandatory registration to ensure
that patients who could become pregnant have negative pregnancy
testing and birth control counseling before receiving the drug.
To inform health care providers about iPLEDGE, FDA has issued a
Public Health Advisory and revised the Patient and Health Care
Provider Information Sheets that detail the tightened restrictions
and increased responsibilities under iPLEDGE for prescribing,
dispensing, distributing, and obtaining isotretinoin.
To obtain the drug, in addition to registering with iPLEDGE,
patients must comply with a number of key requirements that include
completing an informed consent form, obtaining counseling about the
risks and requirements for safe use of the drug, and, for women of
childbearing age, complying with required pregnancy testing.
A reporting and collection system for serious adverse events
associated with the use of istotretinoin has also been implemented.
All pregnancy exposures to isotretinoin must be reported immediately
to the FDA via the MedWatch 1800-FDA-1088 and to the iPLEDGE
pregnancy registry at 1-866-495-0654 or on the iPLEDGE website.
Doctors, patients, and pharmacies can obtain program information
and register with iPLEDGE via the internet, beginning August 22,
2005, at www.ipledgeprogram.com or telephone 1-866-495-0654.
In addition to approving the iPLEDGE program, FDA has approved
changes to the existing warnings, patient information and informed
consent document so that patients and prescribers can better
identify and manage the risks of psychiatric symptoms and depression
before and after prescribing isotretinoin.
Under the program, after October 31, 2005, wholesalers and
pharmacies will have to register with iPLEDGE to obtain isotretinoin
from a manufacturer. Starting December 31, 2005, all patients and
prescribers (doctors) must register and comply with requirements for
office visits, counseling, birth control and other responsibilities.
The manufacturers participating in the iPLEDGE program include:
Hoffman-LaRoche manufacturer of Accutane; Genpharm manufacturer
of Amnesteem which is distributed by Mylan/Bertek; Ranbaxy
Pharmaceuticals manufacturer of Sotret; and Barr Laboratories
manufacturer of Claravis.
BRILLIANT US DISTRICT
JUDGE ISSUES INJUNCTION, USFDA INVESTIGATED THEN
BLOCKS SALE OF ILLEGAL
DRUGS
The U.S. Food and Drug Administration (FDA) today announced a
permanent injunction shutting down operations at Pharmakon Labs of
Florida. The company manufactured and distributed cough and cold
liquids, tablets and caplets.
Following inspections by FDA and a trial in U.S. District Court,
Judge Richard A. Lazzara found that drug products sold by Pharmakon
Labs, Inc., its president Abelardo L. Acebo, and its
secretary/treasurer Edward R. Jackson (the defendants) did not meet
current good manufacturing practice (cGMP) standards and other legal
requirements.
Judge Lazzara stated that he was "simply unwilling as a court of
equity to place the health, safety, and welfare of the general
public at risk in order to accommodate the economic well-being of
Defendants." Thus, the defendants were ordered to stop manufacturing
and distributing drugs until they become compliant with CGMP
standards to the satisfaction of FDA and obtain marketing approvals.
"This action by Judge Lazzara sends a strong signal that FDA will
take action against drugs that fail to meet quality standards," said
FDA Commissioner Dr. Lester M. Crawford. "As the nation's top
enforcer of manufacturing standards, the FDA will continue to ensure
that drugs being sold in this country meet those crucial
requirements."
The defendants have a long history of continued violations of the
Federal Food, Drug, and Cosmetic Act. The government's initial
complaint alleged numerous manufacturing violations documented in
four inspections dating back to 2001. FDA later added charges
related to Pharmakon's manufacture and distribution of unapproved
new drugs, as part of the agency's longstanding policy to seek
relief for all legal violations by a firm at the same time.
The government's request for a permanent injunction was based on
the defendants' demonstrated unwillingness to comply with the law.
FDA ISSUES PUBLIC
HEALTH ADVISORY FOR MIFEPRISTONE
The Food and Drug Administration (FDA) is investigating
recently reported serious adverse events associated with
mifepristone (trade name Mifeprex, also known as RU-486). As a
result, the FDA is issuing a public health advisory today
highlighting the risk of sepsis or blood infection when
undergoing medical abortion using Mifeprex and misoprostol in a
manner that is not consistent with the approved labeling. There
are now four cases of deaths from infection from September 2003
to June 2005 following medical abortion with these drugs.
"The FDA is committed to sharing emerging drug information
with the public and we believe it is important to share with
healthcare providers and patients the latest serious reports of
infection associated with this drug that we have received," said
Dr. Steven Galson, Acting Director of FDA's Center for Drug
Evaluation and Research.
The bacteria thought to have caused the fatal infection have
been identified in two of the cases and the other two cases are
under investigation by FDA along with the Centers for Disease
Control and Prevention, State and local health departments, and
the manufacturer of Mifeprex. Doctors are urged to have a higher
level of suspicion for sepsis in their patients taking Mifeprex.
Previously, the FDA has received reports of serious bacterial
infection, bleeding, ectopic pregnancies that have ruptured, and
death. Those reports led to the revision of the black box
labeling. Mifeprex was approved by the FDA in 2000.
-
FDA Issues Nationwide Alert for "Liqiang 4"
Due to Potential Health Risk
The U.S. Food and Drug Administration (FDA) is warning consumers not
to take Liqiang 4 Dietary Supplement Capsules because they contain glyburide
– a drug that could have serious, life-threatening consequences in some
people.
Glyburide is a drug used to lower blood sugar, and is safe and
effective when used as labeled in FDA-approved medications. People who
have low blood sugar or those with diabetes can receive dangerously high
amounts of glyburide by consuming Liqiang 4. Consumers should
immediately stop using these products and seek medical attention,
especially if they are currently being treated with diabetes drugs or if
they have symptoms of fatigue, excessive hunger, profuse sweating, or
numbness of the extremities. Consumers who have this product should
dispose of it immediately.
The product is sold as part of a shrink-wrapped two bottle set. One
of the 90 capsule bottles is labeled Liqiang 4 Dietary Supplement
Capsules, the other bottle is promoted as a “bonus pack” of Liqiang 1.
At this time FDA is evaluating Liquang 1 and other versions of this line
of products to determine their composition and safety. The product is
manufactured by Liqiang Research Institute, China, and marketed
throughout the United States in herbal stores and through mail order by
Bugle International of Northridge CA.
The FDA learned of the potential problem through an anonymous
consumer complaint and followed up with testing that revealed the
presence of glyburide in this product.
The product has also been termed "Liqiang Xiao Ke Ling" (Liqiang
Thirst Quenching Efficacious) in ads in Chinese language publications
which also promote it as useful for the control of diabetes and being
derived from only natural ingredients.
FDA encourages consumers, health care providers, and caregivers to
report any adverse events related to this product to MedWatch, the FDA's
voluntary reporting program at 1-800-FDA-1088; by FAX at 1-800-FDA-0178;
by mail to MedWatch, Food and Drug Administration, 5600 Fishers Lane,
Rockville, MD, 20857-9787; or online at
www.fda.gov/medwatch/report.htm.
-
FDA Issues Information for Consumers about
Claims for Green Tea and Certain Cancers
Under the Food and Drug Administration's (FDA) "Consumer Health
for Better Nutrition Initiative," the Agency is announcing the
results of a review of qualified health claims that green tea may
reduce the risk of certain types of cancer. Based on a systematic
evaluation of the available scientific data, the FDA intends to
consider exercising its enforcement discretion for the following
qualified health claims for breast and prostate cancer:
"Two studies do not show that drinking green tea reduces the risk
of breast cancer in women, but one weaker, more limited study
suggests that drinking green tea may reduce this risk. Based on
these studies, FDA concludes that it is highly unlikely that green
tea reduces the risk of breast cancer"; and
"One weak and limited study does not show that drinking green tea
reduces the risk of prostate cancer, but another weak and limited
study suggests that drinking green tea may reduce this risk. Based
on these studies, FDA concludes that it is highly unlikely that
green tea reduces the risk of prostate cancer."
The FDA also concluded that existing evidence does not support
qualified health claims for green tea consumption and a reduced risk
of any other type of cancer.
Guidance on qualified health claims for conventional foods and
dietary supplements was issued by the FDA in July 2003. FDA will
continue to evaluate new information that becomes available to
determine whether changes in these claims, or in the decision, are
necessary.
-
ACADEMY NEWS-NEW LIFE
FELLOW
Under
and by virtue of the full authority,
provisions and privileges vested herein,
the American Academy For Justice Through Science
proclaim that in recognition of
her valuable contributions in Ethics,
Outstanding Medicine, and service to the public trust, hitherto Dr.
Marie King PhD FAAJTS CA-#2008, Forensic Clinical Psychologist, life fellowship, full rights, privileges and honors status in the
American Academy For Justice Through Science' as a 2005 Fellow of the
Board.
Congratulations - Press Release
-
LETTER TO THE EDITOR
Some
say that the age of chivalry is past, that the spirit of romance is
dead. The age of chivalry is never past, so long as there is a wrong
left unredressed on earth."
Charles
Kingsley,
Vol., II,
Ch 28: "A
good conscience is a continual Christmas." Ben
Franklin
Dear Dr. Neff,
I've been in contact with the people in Iowa that help victims.
But the problem with my pains
and memory loss was related to
my thyroids
all this time! I
feel deep sadness from what's happened;
eight years wasted,
sometimes it feels weird seeing my
nine grandchildren and not remembering 5 of their births!
You see I had a great
memory and ears like tape recorders. Now part of the gifts that I was born with have
been erased, but the most sadness came...(Editor's
Note: The rest of Paula's statements were simply too personal in
nature relative to her loss of health.).
Thank you for your emails
and good advice.
It's good to know
someone still has a heart!
Paula Nelson-05-21-2005
 -"InfoJustice" -"InfoJustice"
-
ACADEMY NEWS-NEW MEMBERS
Under
and by virtue of the full authority,
provisions and privileges vested herein,
the American Academy For Justice Through Science
proclaim that in recognition of
valuable contributions in Ethics,
Outstanding Medicine, and service to the public trust and the Academy,
hitherto Dr. Alan Dinehart DC MD FAAJTS CA & SC-#2009, full fellowship, rights, privileges and honors status in the
American Academy For Justice Through Science' as a 2005 Fellow of the
Board.
Congratulations - Press Release
-
FDA APPROVES NEW COMBINATION VACCINE FOR
ADOLESCENT AND ADULT WHOOPING COUGH
The Food and Drug Administration (FDA) today approved a new vaccine
for a single booster immunization against pertussis (whooping
cough), in combination with tetanus and diphtheria, for adolescents
and adults 11-64 years of age. The vaccine will be marketed as
Adacel by Aventis Pasteur Limited located in Toronto, Canada. Adacel
is the first vaccine approved as a pertussis booster for adults.
Vaccines for prevention of tetanus and diphtheria (Td vaccine) in
adolescents and adults have been available for many years.
Adacel is a Tetanus Toxoid (T), Reduced Diphtheria Toxoid (d) and
Acellular Pertussis Vaccine (ap), Adsorbed. Adacel contains the same
components as Daptacel, a DTaP vaccine indicated for infants and
children manufactured by Aventis Pasteur Limited, but the diphtheria
toxoid and one of the pertussis components are in reduced quantities.
Recently, FDA approved a similar vaccine called Boostrix,
manufactured by GlaxoSmithKline, for use in adolescents 10-18 years of
age.
Pertussis is a highly communicable and potentially serious illness in
adolescents and adults, and can cause prolonged cough and missed days at
school and work. In young infants, pertussis is more frequently severe
and can be fatal, particularly in those too young to be fully
vaccinated. Since 1980, the rates of reported pertussis cases have been
increasing in adolescents and adults, as well as in young infants.
Adolescents and adults have been implicated as the source of pertussis
infection for susceptible young infants, and other family members.
The ability of Adacel to protect against pertussis was assessed by
comparing the antibody responses of adolescents and adults who received
it with the antibody responses of infants who had received Daptacel in a
clinical trial. The antibody responses of the adolescents and adults who
received a single dose of Adacel were at least as good as those observed
in the infants following three doses of Daptacel. For diphtheria and
tetanus, the antibody responses following Adacel were comparable to
those following immunization with a U.S. licensed Td vaccine.
In clinical trials, the safety of Adacel was compared to a U.S.
licensed Td vaccine. Among adolescent recipients of Adacel, injection
site pain and low grade fever were observed more frequently than among
those who received Td vaccine. Rates of adverse reactions were similar
in adults receiving Adacel vaccine or receiving Td vaccine.
-
FTC PUTS THE SQUEEZE ON TROPICANA'S ORANGE JUICE
CLAIMS
The Federal Trade Commission has settled a
complaint against Tropicana Products, Inc., in which it alleged the
company misled consumers with claims that drinking two to three
glasses a day of its “Healthy Heart” orange juice would produce
dramatic effects on blood pressure, cholesterol, and homocysteine
levels, thereby reducing the risk of heart disease and stroke. Under
the terms of the consent agreement settling the charges, Tropicana
is prohibited from making similar health-related claims in the
future unless they can be substantiated by reliable scientific
evidence.
According to the Commission, Tropicana ran the
“Healthy Heart” ads between 2002 and early 2004, on television and in
publications such as Newsweek magazine. The ads claimed that drinking
two to three cups of Tropicana orange juice each day would lower
systolic blood pressure by 10 points, raise HDL cholesterol by 21
percent and improve the HDL to LDL cholesterol ratio by 16 percent,
increase blood folate levels by 45 percent and lower blood homocysteine
levels by 11 percent. The complaint charges that the benefits were not
substantiated and claims of clinical support for them were false.
“Orange juice contains many nutrients
important to a healthy diet, and advertising can be an important source
of information about the health benefits of foods,” said Lydia Parnes,
Director of the Bureau of Consumer Protection. “But it is essential that
such advertising be truthful. In this case Tropicana’s claims went well
beyond its scientific support.”
According to the Commission, Tropicana ran the
“Healthy Heart” ad as a two-page spread in Newsweek magazine in February
2004. In 2002, Tropicana ran a more extensive national advertising
campaign, including several television commercials and a full-page print
ad in the New York Times, as cited in the Commission’s complaint. The
2002 ad campaign made a claim virtually identical to the 10-point blood
pressure reduction claim that appeared in the 2004 advertising. The
Commission staff had specifically expressed its concerns about the blood
pressure claim made in the earlier campaign in a public closing letter
in July 2002, but did not seek formal agency action at that time. As the
letter noted, although foods that are rich in potassium and low in
sodium such as orange juice have been recognized by public health
authorities, including the Food and Drug Administration (FDA), to help
reduce the risk of hypertension and stroke, the 10-point blood pressure
reduction claim did not appear to be substantiated.
The Commission’s complaint charges Tropicana with
making unsubstantiated claims that: 1) drinking three cups of Tropicana
orange juice a day for four weeks will raise HDL cholesterol by 21
percent and improve the ratio of HDL to LDL cholesterol by 16 percent;
2) drinking 20 ounces of Tropicana orange juice a day will increase
blood levels of folate by almost 45 percent and decrease homocysteine
levels by 11 percent; and 3) drinking two cups of Tropicana orange juice
a day for six or eight weeks will lower systolic blood pressure an
average of 10 points. The complaint also charges that Tropicana’s claims
that clinical studies demonstrated these benefits were false.
The consent order prohibits Tropicana from making
the challenged claims or any similar claims about the effects of orange
juice or other foods on blood pressure, cholesterol levels, folate
levels, and homocysteine levels or other biological markers or
health-related endpoints unless the company substantiates the claim with
competent and reliable scientific evidence. The order also prohibits
claims by Tropicana that any food will have an effect on the risk of
heart disease, stroke, or cancer unless substantiated by competent and
reliable scientific evidence. The order also prohibits any
misrepresentations relating to tests or studies. Tropicana is permitted
under the settlement to make certain claims that comply with specific
FDA regulations for food labeling. Finally, the order contains various
record keeping requirements to assist the FTC in monitoring compliance.
-
HAPPY MEMORIAL DAY; PLEASE
BE CAREFUL AND WATCH
 YOUR KIDS. YOUR KIDS.
Please have a safe and happy holiday. And
may our troop abroad come home safe and soon. Yet, "Memorial Day" is one of those special
holiday's statistically, which has very high incidents of injuries.
Children exited to get into the water for the first time this year, (oceans, lakes, rivers, and
swimming pools) sustain serious neck and spine injuries. These
life threatening injuries can be avoided by becoming aware of the
"holiday psychology in play", advise your children accordingly, and try
to keep a special eye out for accidents. Primarily the water
injuries are sustained by diving and hitting the skull, although other
out door water sports must be supervised such as waterskiing,
surfboarding and the like. If you or your children compete in a
new spring event which requires exercise, warm up, stay out of prolonged
sun exposure, and bring electrolytes or even a combination of the simple
salts such as table salt, and 'kosher for their sodium and potassium
respectively.
If you can prepare "Gator-aid" like drinks, these will be
sufficient.
Consult your family physician for in-depth advise.
With the warmest of hopes, the members of the
American Academy For Justice Through Science wish all Americans, a
happy, healthy, thought
provoking and safe Memorial Day weekend.-"InfoJustice"

-
LETTERS TO THE EDITOR
Dear Dr. Neff,
I was injured and treated by
Doctor who put me on SSI and treated me
as mental patient. My dead line for
finding an attorney is Aug. of this year. Have a
doctor now treating me for posttraumatic...
and can truly say the meds first doctor had me on were not only wrong
but going off the charts. Also
I suffer lots of memory loss.
Is there truly still justice
for the poor or only for those who can afford it?
Dear Paula, I am also from the great
heartlands, and my social mores and sound ethics have proved that today
is one of the most anti-justice, anti-science and anti-truth periods of
the last 50 years. Quackery, fraud, hucksterism and folks who just
don't give a hoot about the truth are very prevalent today. There
are many folks who wish to rip off the insurance industry or steal
money from you when you are ill, disabled or especially on fixed incomes
or poor. There are folks out there only after your money
offering you incorrect medicinal substitutes which you discovered and
described above in laymen's terms, " not only wrong but going off
the charts" .
Be careful with your own health. I will document your case further
should you continue.
Finally, seek out a quality specialist to
assist your new doctor and attorney
by August. Do this by simply calling your states Medical Board and
State Bar and get a referral for an MD and an attorney who specializes
in working within the medicine arena. Take an action step and act
now. If you need more assistance I will do what I can.-"InfoJustice"
-
HUMONGOUS ABLE LABS
RECALL FOR DRUGS WITH TAINTED
ACETAMINOPHEN
Able Laboratories of Cranbury, NJ, is conducting a nationwide
recall of all of its manufactured drugs (mostly generic prescription
drugs, including drugs containing acetaminophen) because of serious
concerns that they were not produced according to quality assurance
standards. Able Laboratories has ceased all current production.
"The FDA continues to evaluate the situation at Able Laboratories to
determine the safety and quality of their products and will update the
public on our findings as necessary," said Margaret O'K. Glavin,
Associate Commissioner for Regulatory Affairs. "In the meantime, the
Agency recommends that people who have been taking drugs produced by
this firm speak with their health care provider or pharmacist to obtain
a replacement drug product. The drug recall
involves well over 150 different drug products which also contain
Acetaminophen. The drugs include such favorites as tablet
Hydrocodone, Codeine, Lithium, Naproxen Sodium, Nitroglycerin
Sublingual, Promethazine, Theophyllyine, and much much more as well as a
list of inhaled and liquid medicines.-"InfoJustice"
- COUNTERFEIT LIPITOR,
VIAGRA AND EVISTA
The Food and Drug Administration has approved Requip (ropinirole) to
treat moderate to severe Restless Legs Syndrome (RLS). The drug was
first approved for Parkinson’s disease in 1997.
Restless Legs Syndrome is a condition that affects about ten percent
of the population. The disorder is characterized by an urge to move the
legs, usually accompanied by or caused by uncomfortable leg sensations.
For most people with the condition, symptoms begin or worsen during
periods of rest or inactivity and are partially or totally relieved by
movement. Symptoms typically worsen or occur only in the evening or at
night, and can disturb sleep.
Requip was found to be effective for RLS in three randomized,
double-blind placebo controlled studies in adults diagnosed with
moderate to severe RLS. The studies measured effectiveness of the drug
using the International Restless Leg Syndrome Scale, a patient rated
scale that measures different aspects of RLS including severity of
muscle movement and discomfort, sleep disturbance, mood and overall
effect on quality of life. The Clinical Global Impression-Global
Improvement scale was also used. This is an investigator rated scoring
of improvement following treatment. All three studies demonstrated a
statistically significant difference between the treatment group
receiving Requip and the group receiving placebo.
Common side effects of Requip reported in clinical trials include
nausea, headache, and vomiting. The label for the drug will also include
a caution that Requip has been associated with sedating effects,
including somnolence (sleepiness), and the possibility of falling asleep
while engaged in activities of daily living, including operation of a
motor vehicle. Syncope (fainting) or symptomatic hypotension (low blood
pressure) may occur, particularly during initial treatment or dosing.
FDA APPROVES REQUIP FOR RESTLESS LEGS SYNDROME
The Food and Drug Administration has approved Requip (ropinirole) to
treat moderate to severe Restless Legs Syndrome (RLS). The drug was
first approved for Parkinson’s disease in 1997.
Restless Legs Syndrome is a condition that affects about ten percent
of the population. The disorder is characterized by an urge to move the
legs, usually accompanied by or caused by uncomfortable leg sensations.
For most people with the condition, symptoms begin or worsen during
periods of rest or inactivity and are partially or totally relieved by
movement. Symptoms typically worsen or occur only in the evening or at
night, and can disturb sleep.
Requip was found to be effective for RLS in three randomized,
double-blind placebo controlled studies in adults diagnosed with
moderate to severe RLS. The studies measured effectiveness of the drug
using the International Restless Leg Syndrome Scale, a patient rated
scale that measures different aspects of RLS including severity of
muscle movement and discomfort, sleep disturbance, mood and overall
effect on quality of life. The Clinical Global Impression-Global
Improvement scale was also used. This is an investigator rated scoring
of improvement following treatment. All three studies demonstrated a
statistically significant difference between the treatment group
receiving Requip and the group receiving placebo.
Common side effects of Requip reported in clinical trials include
nausea, headache, and vomiting. The label for the drug will also include
a caution that Requip has been associated with sedating effects,
including somnolence (sleepiness), and the possibility of falling asleep
while engaged in activities of daily living, including operation of a
motor vehicle. Syncope (fainting) or symptomatic hypotension (low blood
pressure) may occur, particularly during initial treatment or dosing.
MARGARET
O'K.
GLAVIN AS NEW ASSOCIATE USFDA COMMISSIONER FOR REGULATORY AFFAIRS
John M. Taylor, III, U.S. Food and Drug Administration's (FDA's)
Associate Commissioner for Regulatory Affairs, today announced his
decision to leave FDA after a distinguished 14 year career at the
agency. Margaret O'K. Glavin, FDA's current Assistant Commissioner in
the Office of Counterterrorism Policy and Planning, has been named the
new Associate Commissioner.
"As the head of our field force, John championed the public health by
bringing some of the agency's largest and most significant enforcement
actions," said Dr. Lester M. Crawford, Acting FDA Commissioner. "Indeed
John's legacy at the agency includes significant accomplishments related
to agency initiatives on blood safety, counterterrorism, food safety and
pharmaceutical product quality."
Mr. Taylor joined FDA's Office of the Chief Counsel in 1991 after
graduating from the law school of the College of William & Mary. Six
years later he moved to the Office of the Commissioner as Senior Advisor
on Regulatory Affairs. In 2000, he was named Director, Office of
Enforcement, in FDA's Office of Regulatory Affairs, and served in that
capacity until his appointment to his current position in 2002.
Prior to FDA, Ms. Glavin served at the U.S. Department of Agriculture
as Acting Administrator of the Food Safety and Inspection Service (FSIS),
a 10,000-person public health regulatory agency responsible for the
safety of the meat and poultry supply. Before being named Acting
Administrator in 2001, Ms. Glavin served as Associate Administrator of
FSIS, a position in which she was responsible for the daily operations
of that agency and its 7,000-person field force. Immediately prior to
joining FDA in 2003, Ms. Glavin spent a year focusing on food safety
issues as a visiting scholar at Resources for the Future, a prominent
Washington, D.C. think tank.
"Maggie brings extensive leadership experience and a background in
crisis management to this very important position at FDA," added Dr.
Crawford. "The work of our field force is absolutely critical to our
public health mission."
A graduate of Trinity College and Georgetown University, Ms. Glavin
has published articles in various publications, including Food and
Agriculture 2003, SAIS Review, and Food and Drug Law Journal.
Boris D. Lushniak, MD, MPH, will replace Ms. Glavin as the FDA's
Assistant Commissioner for Counterterrorism Policy. Dr. Lushniak
previously served as the Chief Medical Officer in the FDA's Office of
Counterterrorism Policy and Planning. Dr. Lushniak is a Captain in the
Commissioned Corps of the U.S. Public Health Service who has significant
expertise in counterterrorism activities, disaster response, medical
epidemiology and occupational diseases.
Members: The membership has
been invited to attend a interesting conference for International
Members of the Academy for Justice Through Science. The invitation;
The Forensic
Institute...&...are presenting, as part of
their ... conference series, the 1st
International Human Identification...Symposium.
This International... Conference will be held...on
the 14 April 2005 and you are invited to register for the...Symposium
free of charge.
The theme of the...Symposium - 'Bridging
the Gap between Science and Law' -addresses one of the most pressing
challenges the scientific, law enforcement and legal communities face
today. This high profile event aims to stimulate and feed this triangle
of the scientific, law enforcement and legal communities with cutting
edge knowledge delivered by world-renowned speakers.
I would most appreciate inclusion in
your event calendar and on your web site, if at all possible.
Kind regards,
...
Note:
Confidentiality: This e-mail and its attachments are intended for the
above named recipient's only and may be
confidential and/or privileged. If they have come to you in error you
must take no action based on them, nor must you copy or disclose them or
any part of their contents to any person or organization...
Contact the American Academy For
Justice Through Science home office for dates, and times.-"InfoJustice"
AMERICAN
ACADEMY OF CHILD AND ADOLESCENT PSYCHIATRY
FOR CHILD AND ADOLESCENT
PSYCHIATRISTS
REGARDING THE FDA
BLACK BOX WARNING ON THE USE OF ANTIDEPRESSANTS FOR PEDIATRIC
October 31, 2004
In making a decision affecting the health of our
children who have psychiatric disorders, the FDA, of necessity, had to
accept the very limit of available data, and in some aspects had to
extrapolate entirely beyond available information.
The FDA’s public health program on antidepressant
medication use in children and adolescents now requires that
pharmaceutical manufacturers place a black box in each
antidepressant’s package insert. The warning is about increased
suicidal thinking and suicidal behavior that can occur in children and
adolescents during the early phases of treatment.
Suicidality in Children and
Adolescents
Antidepressants increase the risk
of suicidal thinking and behavior (suicidality) in children and
adolescents with major depressive disorder (MDD) and other psychiatric
disorders. Anyone considering the use of [Drug Name] or any other
antidepressant in a child or adolescent must balance this risk with
the clinical need. Patients who are started on therapy should be
observed closely for clinical worsening, suicidality, or unusual
changes in behavior. Families and caregivers should be advised of the
need for close observation and communication with the prescriber.
[Drug Name] is not approved for use in pediatric patients except for
patients with [Any approved pediatric claims here]. (See Warnings and
Precautions: Pediatric Use)
Pooled analyses of short-term (4 to 16 weeks) placebo-controlled
trials of nine antidepressant drugs (SSRIs and others) in children and
adolescents with MDD, obsessive compulsive disorder (OCD), or other
psychiatric disorders (a total of 24 trials involving over 4400
patients) have revealed a greater risk of adverse events representing
suicidal thinking or behavior (suicidality) during the first few
months of treatment in those receiving antidepressants. The average
risk of such events on drug was 4%, twice the placebo risk of 2%. No
suicides occurred in these trials.
The FDA advisory panels, which met in September
2004, became concerned that physicians’ variable prescribing practices
for these antidepressant medications might increase any potential
problem. It should be noted that the data on which the concern was
based was derived from clinical trials where clinical standards were
optimal. There is no evidentiary basis for believing that current
practices are contributing to any significant public health problem.
To the contrary, the increase in SSRI prescriptions has been
correlated with a decrease in the youth suicide rate, and consecutive
autopsies have failed to demonstrate the presence of a significant
number of suicides with evidence of SSRI exposure.
The FDA followed several of the AACAP
recommendations in the language and intent of the black box warning.
These included the decision to require that a medication guide (Medguide)
be distributed with each supply of antidepressant medication. This
guide lays out specific warning signs of antidepressant side effects
in lay language for parents.
The FDA black box noted the serious impairments
of untreated depression as well as the newly discovered low risk of
suicidal thoughts. It also called for more research on the long-term
effectiveness of antidepressants. It is important to note that the FDA
did not assert that the use of these medications in children and
adolescents with depression was contraindicated, so physicians can
continue to prescribe them.
What new research
data actually support the FDA’s decision to use a black box warning?
Pooled
analyses of short-term (4 to 16 weeks) placebo-controlled trials of
nine antidepressant drugs (SSRIs and others) in children and
adolescents with major depressive disorder (MDD), obsessive compulsive
disorder (OCD), or other psychiatric disorders (a total of 24 trials
involving over 4,400 patients) have revealed a greater risk of adverse
events representing suicidal thinking or behavior (suicidality) during
the first few months of treatment in those receiving antidepressants.
It should be noted that only 78 of the 4,400 patients experienced
suicidal thinking or suicidal behavior, and no suicides occurred in
these trials. The average risk of such events on a drug was 4
percent, twice the placebo risk of 2 percent.
What unintended
effects on practice might occur following the FDA’s issuing a black
box?
Probably this warning will discourage the
capricious prescribing of these drugs, eliminate direct-to-consumer
advertising, and stop physicians from distributing drug samples. The
warning may also keep depressed patients from seeking treatment. The
black box warning also may cause physicians to avoid treating
depressed children and adolescents because of fear of potential
lawsuits. The Work Group on Research recommends that professional
organizations support their members with open, strong statements about
the value of this treatment.
How frequently
do the research data suggest I would encounter this risk in my
practice if I treat children and adolescents with antidepressants?
The FDA
research has shown that there is a small increase in risk of suicidal
ideation or suicidal behavior in children and adolescents treated with
antidepressants. This effect represents a 2 % increase over that
created by the use of a placebo. That means that if you institute
medication treatment in 200 new patients, you will see approximately 8
child and adolescent patients with increased suicidal ideation or
suicidal behavior. Four of those patients will have experienced these
increased symptoms as part of their depression, while the remaining
four may have increased ideation or suicidal behavior related to
antidepressant treatment. It should be noted that both
suicidal ideation and suicide attempts are very common in adolescence
and do not have the same prognostic significance for completed
suicide as those behaviors in later life. Thus, the annual
prevalence of attempts in the U.S. is about 10 times greater than the
prevalence of depression. Based on the most recent data, there are 370
attempts for every suicide among teen males and around 3,600 attempts
among teen females each year for every suicidal death.
What do the
research data suggest about the efficacy of antidepressants for
treating depression in children and adolescents?
New research, such as the Treatment for
Adolescents with Depression Study (TADS), confirms that using
cognitive behavioral therapy (CBT) - a type of psychotherapy that
focuses on managing negative emotions and thoughts - and fluoxetine
(Prozac) results in successful treatment of moderate-to-severe
adolescent depression. Seventy-one percent of the patients responded
positively to the combination treatment of fluoxetine and therapy,
which is a rate double the 35 percent response rate for patients on
placebo. Over 60 percent of those assigned to fluoxetine alone were
found to be responders by the end of the 12-week trial.
This means that on average each practitioner
would need to treat just three patients to see a strong response to
fluoxetine. This is in contrast to the need to treat over 50 patients
in order to see evidence of the medication causing suicidal ideation
or suicidal behavior. The Work Group on Research finds this
risk-benefit ratio for the treatment of pediatric depression
acceptable for child and adolescent patients.
How does the AACAP
Work Group on Research recommend that I treat my child and adolescent
patients with depression?
The Work Group continues to advise the child and
adolescent psychiatrists in the AACAP to continue to treat with
psychotherapy or antidepressants or the combination based on the
available research evidence. The research evidence available to the
FDA shows that fluoxetine, now the only SSRI antidepressant available
as a lower-cost generic, has shown efficacy in the treatment of
children and adolescents with depression and with OCD. Because of the
data available, the Work Group recommends that fluoxetine alone, CBT
alone or fluoxetine plus CBT be considered as first line treatment
approaches for depressed pediatric patients. The Work Group also
recommends that patients be monitored with the frequency of visits
suggested by the FDA; although, there are no specific research data to
support the frequency of face-to-face contacts.
What if I receive a
referral for a child or adolescent who has failed on fluoxetine? Can I
still treat with an alternative antidepressant?
The FDA did not contraindicate the use of any of
the other SSRI antidepressants. Although there were some differences
in the degree of risk among the nine antidepressants evaluated, the
agency did not find compelling evidence to contraindicate any of the
drugs with a higher than usual risk for the suicidal ideation or
suicidal behavior, or, conversely, to not apply the black box warning
to any antidepressant with a low risk rate. For that reason, the Work
Group on Research would recommend considering any of the other SSRIs
that the practitioner has had success with in other pediatric patients
with depression.
What should I do if
my child or adolescent depressed patient shows increased suicidal
ideation or increased rates of suicidal behavior?
The Work Group reminds practitioners that they
should take all steps necessary to protect the well being of their
patients. In patients whose depression is persistently worse, or who
are experiencing emergent suicidality, consideration should be given
to changing the therapeutic regimen, including reducing the dose of
the antidepressant, and possibly discontinuing the medication. Drug
discontinuation should be considered if these symptoms are severe,
abrupt in onset, or were not part of the patient's presenting
symptoms. Any discontinuation should be done carefully to prevent
adverse events that may occur after abrupt antidepressant
discontinuation. Doses should be tapered rather than an abrupt
stoppage, particularly if the medication is an SSRI other than
fluoxetine.
In the new FDA
labeling, which recommendations lack research support and may not
protect my patients from these side effects?
The new FDA labeling in the warnings and
precaution section contain a number of suggestions that have yet to be
supported by an adequate amount of research. For that reason, the
AACAP Work Group on Research does not consider the factors listed
below should be given more weight than other clinical issues in making
treatment decisions.
► Family history of bipolar disorder is
not a reliable warning sign a patient will experience these side
effects. The FDA recommends that bipolar disorder be ruled
out before treating children and adolescents with antidepressants.
Although this warning is called a precaution, it is not a
contraindication. The FDA suggested labeling language states, “It is
generally believed (though not established in controlled trials) that
treating such an episode with an antidepressant alone may increase the
likelihood of precipitation of a mixed/manic episode in patients at
risk for bipolar disorder.” Although the label states that “such
screening should include a detailed psychiatric history, including a
family history of suicide, bipolar disorder, and depression,” these
factors were not shown to be predictive of increases in suicidal
ideation or suicidal behavior in the FDA reviews. While the Work Group
on Research agrees that a thorough evaluation should be done on each
patient, the value of this data in guiding the decision of whether or
not to treat with SSRIs is not established, and we do not believe such
a history should preclude use of these agents beyond the caution of a
“switch” from depression to mania or hypomania.
If there is a positive family history of bipolar disorder, a
careful diagnostic assessment should be done to consider the
possibility that the patient is not in the depressed phase of a
bipolar illness. The risk of giving antidepressants to someone in the
depressed phase of bipolar illness or a mixed episode is that the
medication may switch the patient into a manic state, at least
according to experience with adult bipolar patients. There are no
definitive databased strategies for how best to treat depressed
patients at genetic risk for bipolar disorder, including those
patients who are at increased risk for developing bipolar disorder in
the future.
►
Suicidal ideation or suicidal behavior does not
always follow other SSRI side effects.
The FDA label strongly hints that standard SSRI side effects
may be precursors of suicidal ideation or suicidal behavior, and
advises clinicians and parents to monitor for them without evidence
that they are precursors for increased suicidal ideation or suicidal
behavior. The new labeling states that “anxiety, agitation, panic
attacks, insomnia, irritability, hostility (aggressiveness),
impulsivity, akathisia (psychomotor restlessness), hypomania, and
mania, have been reported in adult and pediatric patients being
treated with antidepressants for major depressive disorder as well as
for other indications, both psychiatric and non-psychiatric.” These
should be tracked, even though “a causal link between the emergence of
such symptoms and either the worsening of depression and/or the
emergence of suicidal impulses has not been established.” The Work
Group on Research, while supporting the FDA’s concern over these side
effects, does not agree that there are adequate data yet to support
the FDA’s “concern that such symptoms may represent precursors to
emerging suicidality.” The Work Group on Research does urge a
discussion with patients and parents about the effects and side
effects of SSRI medication and the natural or expected course of major
depression. This will prepare them for managing the depressive
thoughts that may persist after other symptoms resolve. It will also
help them manage any symptoms of akathisia, insomnia, or other
antidepressant side effects that may occur.
► The effectiveness of
a weekly monitoring program with face-to-face visits has yet to be
proven. The FDA recommends a specific monitoring frequency
for physicians when starting SSRI therapy. The FDA recommends that
observation for clinical worsening, suicidality, or unusual changes in
behavior during the initial few months of anti- depressant drug
therapy “ideally would
include at least weekly face-to-face contact with patients or their
family members or caregivers during the first four weeks of treatment,
then biweekly visits for the next eight weeks, then as clinically
indicated beyond 12 weeks. Additional contact by telephone may be
appropriate between face-to-face visits.” The AACAP Work Group on
Research does not know of evidence that this frequency of visits is
any better than phone contact with the family on a weekly basis with
biweekly face-to-face visits during the first month of treatment.
The
optimal frequency of visits is an empiric question worthy of testing.
Until those research findings become available, practitioners should
attempt to follow the FDA frequency of monitoring guidelines.
► The FDA did not
recommend a standardized rating form or side effect questionnaire for
the practitioner to follow that would include the important concerns.
The AACAP Work Group on Research is
aware that two NIMH research projects now include forms with standard
questions about important side effects that can be administered on a
weekly basis. Forms such as these could prove to be effective in
clinical care.
What is the
downside of not using antidepressant medications to treat my child and
adolescent patients with depression?
The
NIMH TADS did not find an advantage of cognitive behavioral therapy (CBT)
alone over placebo in the short term. However, CBT has been shown to
be effective in other treatment studies of depression in children and
adolescents. For that reason, effective treatment may include CBT or
other evidence-based psychotherapies alone or with the antidepressant
fluoxetine as a first-line treatment for depression. In particular,
psychosocial treatment has been shown to have a protective effect
against suicidal behavior or ideation when combined with
antidepressant medication.
Why should
childhood depression be treated with medications that carry any risk
at all?
The
AACAP Work Group on Research strongly supports the treatment of
children and
adolescents with depression despite risks. Pediatric
depression is a real illness, with neurobiological underpinnings.
Effective treatments for this disorder are available. Although
antidepressant treatment carries risks, untreated depression has
potentially greater risks, and treatment is effective, especially when
started early. Depression is a serious illness, sometimes episodic and
often chronic, when it occurs in childhood. In addition to the human
suffering that occurs because of the depression, the symptoms can and
do interfere with academic learning, peer relationships, and family
interactions, often derailing normal development.
Follow-up studies have shown a higher than normal
rate of serious mental disorder in adult life and shortened mortality
in those with childhood- or adolescent-onset depression. There are
about 1.7 million suicide attempts per year and about 60 percent of
those have a depressive or anxiety diagnosis. Because of the severity
of the disorder, the Work Group on Research supports treatments that
have been shown to be effective in easing the depression and allowing
normal development. The 2004 NIMH TADS study has confirmed that the
SSRI fluoxetine, alone or in conjunction with CBT psychotherapy, is an
effective treatment for youth-onset depression.
What other steps
is AACAP taking to support its members?
The
AACAP plans to expedite the update on the practice parameter for
depression and to distribute it in 2005. AACAP will also revise
relevant Facts for Families to provide practitioners with suitable
materials to hand out in the office. AACAP members are contributing
to other projects to be included in a practice toolkit, including this
letter, a model parental consent form, and a rating form to track the
adverse events in antidepressants, such as increased suicidal ideation
and suicidal behavior. The sample letter to parents or guardians that
is enclosed will also be part of the toolkit.
Sample
Letter to Families:
Explaining the FDA warnings about
antidepressants
October 2004
Dear
Parent/Guardian,
You may have
heard media reports on concerns about prescribing antidepressant
medication for children and adolescents. The reports describe the
meeting at the Food and Drug Administration (FDA) in September 2004 to
review the studies of children and adolescents taking antidepressants.
The agency reviewed studies of depression and anxiety disorders, and
an advisory committee discussed the effectiveness of these
medications, as well as the concerns about increased risk of suicidal
behavior in children and adolescents while taking the medications.
This letter will explain some of the information and answer questions
that you may have.
What did the
FDA Advisory Committee determine?
After two days of
hearings, the advisory committee determined that there is some
increased risk of suicidal behavior for some children or adolescents
taking antidepressants. About 3-4% of children or adolescents with
depression who took an antidepressant had some type of suicidal
behavior (such as a suicide attempt or suicidal thoughts), while 1-2%
of those taking placebo (inactive pill) did. Therefore, there was
almost a 2-fold increase in suicidal behavior in youth taking an
antidepressant to treat their depression. There were NO completed
suicides in any of these studies, which included over 4,000 children
and adolescents. For those with an anxiety disorder, there was no
difference in suicidal behavior in those being treated with
antidepressants as compared to placebo.
The FDA advisory
committee recommended that a stricter warning label be placed on all
antidepressants. The type of warning label they recommended is called
a “black box,” which means any doctor prescribing one of these
medications has to clearly warn patients and their families about the
risks associated with the medication. In this instance, the black box
warns that there is a chance of increased risk of suicidal thoughts
and behaviors in youth taking these medications. Although there were
some minor differences between the various medications evaluated, the
advisory committee decided that the same warnings should be given for
all antidepressants.
How does this
affect your child?
If your child is
already being treated with one of these medications and is doing well,
then your child should continue on the treatment. In most cases, these
increased risks occur during the first weeks of treatment. If your
child has recently started one of these medications or is about to
start, then you and your doctor will need to closely monitor him/her
for any changes in behavior.
Suicidal thoughts
are a symptom of depression. Additionally, depression is one of the
largest risk factors for suicide. It is difficult to interpret whether
suicidal thoughts and behaviors in depressed individuals are due to
the illness itself or the medication. It can be either of these. In
some people, antidepressant medications may increase these types of
thoughts, so this warrants close monitoring for all patients.
It is important
to note that, in the studies, 9% of adolescents in the general
population make a suicide attempt, 3-4% had some suicidal behavior.
What should
you do?
First, be upfront
and honest with your child about these risks. Second, talk to your
child or adolescent about whether they are having any suicidal
thoughts, and let them know they should come to you if they start
having such thoughts. Third, you, your child, and your child’s doctor
should develop a safety plan for your child. This can include
identifying an adult your child can call if he/she is thinking about
suicide. Finally, you and your doctor should closely monitor your
child for the first weeks of treatment. All child and adolescent
patients beginning medication should be seen weekly for the first
month, every other week for the second month, and at least once a
month for the third month by the treating psychiatrist to closely
monitor depressive symptoms and any problems. It is important that you
do not change the dose of your medication without first discussing the
change with your doctor.
What should I
look for?
Be on the look
out for certain behaviors that appear for the first time, seem worse,
or worry your child or adolescent or you. These include new or more
thoughts of suicide, trying to commit suicide, new or worse
depression, new or worse anxiety, or feeling very agitated or
restless. If these appear, a medical professional should be contacted
right away.
If you have any
questions about this information, ask your doctor, who will answer all
other questions you or your child have.
We hope that this
information answers your questions.-InfoJustice
-
CRIMINAL JUSTICE
PSYCHIATRIST JOINS THE ACADEMY
Dr. James Drury DO is a Forensic
Child/Adolescent/Adult Psychiatrist, who presently is
heading up a New Jersey Juvenile Psychiatric Corrections Program.
Psychiatric Director-ConCEPT Program-New Jersey Training School for
Boys-Jamesburg, NJ
Responsible for the evaluation and care of
children in a Medium Security Facility under the auspices of the New
Jersey Juvenile Justice Commission. The patients in this specialized
unit have multiple psychiatric and behavioral problems which have caused
them to be readmitted multiple times into the Juvenile Justice setting.
The focus of the program is to help intervene intensively through the
use of behavioral/emotional/educational techniques to help prevent
recidivism. Responsible for psychiatric/forensic evaluations,
psychotherapy, behavioral interventions, and the prescription of
medications. Serve as the sole psychiatrist to this population which
includes being on-call 24 hours per day, seven days a week. Supervise a
staff of, 2-3 social workers and 9-12 behavioral care specialists and
also testify at commitment hearings for transfer to the state hospital
if warranted by patient’s behaviors. This program is the first of its
kind in the country and is subsidized by both Federal and State grants.
It is believed that this program will become the measure by which other
such programs in the state as well as in the nation are gauged. The
program seeks not only to address the special needs of its clients buy
also to educate the general population of the benefits of such intensive
treatment and supervision.
7/02 to date:
Lead Psychiatrist-New Jersey Juvenile Justice Commission
Responsible for psychiatric/forensic
evaluations, psychotherapy, behavioral interventions, and the
prescription of medications at the state’s medium security juvenile
facilities at both the Jamesburg and Bordentown Campuses, as well as the
Boot Camp. Serve as the sole psychiatrist to this population which
includes being on-call 24 hours per day, seven days a week. Supervise a
staff of 4-5 nurses, 4-5 social workers and also testify at commitment
hearings for transfer to the state hospital if warranted by patient’s
behaviors. Also, responsible for referrals for substance abuse and other
specialized program follow-up and treatment when discharged from the
facility to address the individual child’s special needs.
7/02 to date Consulting Psychiatrist-St. Peter’s
University Hospital
New Brunswick, NJ
Consultant for an
inpatient psychiatric facility serving adult and geriatric populations.
Recommend therapy, pharmacology, and behavioral intervention options.
4/00 to date Police Surgeon/Board of
Directors-AMTRAK Police Fraternal Order of Police
Responsible for the
psychiatric care and counseling of the members of a federal police force
and their families. Duties include medication evaluation, therapy, and
screenings for mental illness. Involved in the establishment of
protocols and procedures for the implementing of these programs as a
member of the Board of Directors.
7/00 to 7/02 Psychiatric Director-Fayette County Prison
Uniontown, PA
Responsible for psychiatric/forensic
evaluations, psychotherapy, behavioral interventions, and the
prescription of medications in an approximately 200-bed rural county
prison facility with an average stay of two years or less. Serve as the
sole psychiatrist to this population which includes being on-call 24
hours per day, seven days a week. Supervise a staff of 4-5 nurses and
also testify at commitment hearings for transfer to the state hospital
if warranted by patient’s behaviors. Also, responsible for referrals for
substance abuse follow-up and treatment when discharged from the
facility.
7/00 to 7/02 Child/Adolescent/Adult
Psychiatrist-Chestnut Ridge Counseling Services, Inc.
Uniontown, PA
Responsible for the psychiatric care and treatment of
outpatient psychiatric patients in a rural mental health
center. This includes psychotherapy, behavioral
interventions, family therapy, and prescribing medications. This
position includes provision of similar services to an Adult Outpatient
Dual Diagnosis Partial Hospitalization Program.
7/00 to 7/02 Consulting
Psychiatrist-Highlands Hospital
Connellsville, PA
Consultant for an
inpatient psychiatric facility serving adult and geriatric populations.
Recommend therapy, pharmacology, and behavioral intervention options.
7/98 to 7/00 Child and
Adolescent Fellow/Assistant Clinical Instructor, East Carolina
University School of Medicine
Greenville,
NC
Responsible for the
care and treatment of pediatric and adolescent psychiatric patients in
outpatient, inpatient, substance abuse, and forensic settings. Duties
included medication evaluation, psychotherapy, emergency room
screenings, and consultations to other psychiatric services.
The list of Dr. Drury's association with law enforcement, various
medical associations and academy's is vast.
The American Academy For Justice Through Science
welcomes
 Dr. Drury to
our "team", and appreciate in anticipation any
consumer advocacy writings, or consumer advice Dr. Drury contributes in
his area of expertise. Welcome Dr.
James A B Drury DO, Forensic Psychiatrist and consumer advocate. Dr. Drury to
our "team", and appreciate in anticipation any
consumer advocacy writings, or consumer advice Dr. Drury contributes in
his area of expertise. Welcome Dr.
James A B Drury DO, Forensic Psychiatrist and consumer advocate. . .
Dear Dr. Neff: I've been searching for information about the murder
case of JonBenet Ramsey, because I have a research paper to write on the
effect it had on America. I can't find the information that I need and
was hoping you could help me out. And this this paper is very important
for my req. for graduation. I was only 10 yrs old when she died so I'm
not very educated on how it impacted other Americans. If you don't have
any info or know of some other site that might I would be so very
grateful if you would help me out.
Dear Andrea (lilchick), Somewhere
on the Beat the Press page is a short forensic analysis that I did on
that case. However, the Crime Library
http://www.crimelibrary.com/ramsey/ramseymain.htm
has
an interesting take on this case. Another comprehensive report was done
by The Encyclopedia of Crime by Crime Magazine. This can be found
http://crimemagazine.com/jonbenet.htm This should start your mystery
solving juices flowing. Good Luck
InfoJustice
September is National Menopause
Awareness Month!
Menopause and Hormones: "What Can You Believe"
Campaign Spearheaded by FDA's Office of Women's Health
The Food and Drug Administration (FDA) is implementing a nationwide
information campaign to raise awareness about the resources available to
address questions related to the benefits and risks of hormone therapy
for menopausal symptoms. According to Census data from 2000, there are
about 37.5 million women reaching or currently at menopause (ages 40 to
59). FDA wants women to be informed about new and emerging safety
information about menopausal hormone treatment.
"Menopausal hormone therapy like all medications has benefits and
risks which is why it is important for FDA to provide the latest, most
helpful information to assist women in making the best decision to fit
their needs," said Dr. Susan Wood, Assistant Commissioner of FDA's
Office of Women's Health. She continued, "FDA's main message is: If you
choose to use hormones for treating symptoms of menopause, use them at
the lowest dose that helps for the shortest time needed."
The FDA and its partners are working to distribute education
materials to help women make informed decisions about their health.
These materials address questions of concern to perimenopausal and
menopausal women considering the use of hormone therapy for relief of
their symptoms. This science-based information has been developed in
collaboration with the National Institutes of Health and other agencies
of the Department of Health and Human Services.
The campaign helps clarify the National Institutes of Health findings
from their landmark Women's Health Initiative (WHI) studies about the
benefits and risks of menopausal hormone therapy. This research
dramatically changed the previous knowledge base about use of hormone
therapy. Women now have questions about what these findings mean for
them. The conclusions from WHI clinical studies showed that women using
estrogen with or without progestin may increase their chances of strokes
and blood clots. Using estrogen with progestin also increased a woman's
chance of getting breast cancer and heart attacks, but using estrogen
alone did not. For women with a uterus on hormone therapy, a combination
of estrogen plus progestin is prescribed. Progestin prevents the
overgrowth of the lining of the uterus, which can lead to cancer, a
known risk of estrogen. For women who have had a hysterectomy, hormone
therapy consists of estrogen alone. Using estrogen with or without
progestin may increase the risk of dementia in women age 65 years or
older. Estrogen, either alone or with progestin, decreased women's
chances of developing weak bones. Estrogen with progestin decreased the
risk of colorectal cancer in women.
Some of the important questions answered in the FDA education
materials include examples such as:
"What are the benefits of using hormones for menopause?" Menopausal
hormone therapy is the most effective FDA approved medicine for relief
of hot flashes, night sweats, and vaginal dryness. For some women,
menopausal hormone therapy may also reduce the chances of getting weak
bones, a condition called osteoporosis. (For women at high risk of
osteoporosis, other medications to prevent bone loss should be
considered.)
"What are the risks of using hormones?"
For some women, menopausal hormone therapy may increase their chances
of getting blood clots, heart attacks, strokes, breast cancer, and gall
bladder disease. For a woman with a uterus, estrogen alone slightly
increases her chance of getting endometrial cancer (cancer of the
uterine lining).
The FDA continues to initiate information and education outreach
activities regarding hormone therapy for menopause. Materials, such as
printable brochures and a list of questions to take to doctor visits,
are downloadable directly from the Internet at the following website
location,
www.fda.gov/womens/menopause/. In conjunction with help from its
national partners, FDA's English and Spanish hormone therapy materials
will help women:
- To know that menopause is normal, and that all women go through it
- To know what is available to them as they go through menopause
- To increase their understanding of menopausal hormone therapy for
treatment of their symptoms.
- To make an informed decision with their doctor, nurse or
pharmacist about ways to manage their menopausal symptoms
The FDA website lists informational resources, such as government
agencies, private organizations, newsletters, magazines, and reports for
women seeking more information about menopause at the following
location:
www.fda.gov/cder/drug/infopage/estrogens_progestins
Further information can be located on the Internet at
www.4women.gov/Menopause/resources.htm. Organizations wishing to
partner with the FDA, or those who wish to order English or Spanish
materials may contact the National Women's Health Information Center (NWHIC)
at (800) 994-9662. NWHIC is a service of the HHS Office of Women's
Health.
The FDA, an agency of the Department of Health and Human Service (HHS),
has partnered with other HHS agencies, as well as not for profit women's
health organizations and professional associations. Currently, there are
approximately 30 FDA partners helping to increase women's awareness
about the use of menopausal hormone therapy.
Susan F. Wood, PhD, Assistant Commissioner for Women's Health, FDA
Office of Women's Health, and Joseph Kaczmarczyk, DO, MPH, Medical
Officer, FDA Office of Women's Health, are available as part of National
Menopause Awareness Month, to discuss the benefits and the risks of
using hormones for menopause and provide helpful resources to women
concerning FDA's campaign.
To schedule an interview with either Dr. Wood, or Dr. Kaczmarczyk,
contact Alice Fisher at 1-800-565-0770.
The U.S. Food and Drug Administration's Office of Women's Health (OWH)
serves as a champion for women's health. It monitors progress of
priority women's health initiatives within the FDA; It promotes an
integrative and interactive approach regarding women's health issues
across all the organizational components of the FDA; and it forms
partnerships with government and non-government entities, including
consumer groups, health advocates, professional organizations, and
industry, to promote FDA's women's health objectives.
FDA Approves New Extended Release Pain
Medication:
Agency Works with Sponsor to Develop an Effective
Plan to Reduce Inappropriate Use
The Food and Drug Administration (FDA) announced today the approval
of Palladone (hydromorphone hydrochloride) capsules for the management
of persistent moderate to severe pain in patients requiring continuous
around-the-clock opioid pain relief for an extended period of time.
Palladone is an extended-release formulation that comes in 12, 16,
24, and 32 milligram (mg.) capsules. This drug should only be used in
patients who are already receiving opioid therapy and who require a
total daily dose of at least 12 mg. of oral hydromorphone or its
equivalent. Palladone offers a therapeutic choice for opioid-tolerant
patients who might otherwise be candidates for other opioids and who do
not achieve satisfactory therapeutic results with these other products.
The active ingredient in Palladone, hydromorphone, is currently a
Scheduled II controlled substance, which is the highest level of control
for drugs with a recognized medical use. Based on the risks associated
with the drug, including the potential for abuse of Palladone, FDA has
worked with the sponsor to develop a comprehensive risk management
program (RMP).
The RMP was designed with three potential risk situations identified.
These are the risks posed by improper dosing, indication, or patient
selection; the risk posed by accidental pediatric exposure to the drug;
and the risk posed by abuse or diversion of Palladone Capsules.
As a controlled substance in Schedule II of the Controlled Substances
Act (CSA), Palladone also comes under the jurisdiction of the Drug
Enforcement Administration (DEA), which administers the CSA. Schedule II
drugs are subject to manufacturing quotas set by DEA with input on
medical need from FDA, distribution tracking, import and export
controls, registration of prescribers and dispensers, and written
prescriptions without refills.
In addition to the protection afforded patients through the status of
Palladone as a controlled substance, the RMP includes provisions for
clear and appropriate labeling, and appropriate education of healthcare
professionals, patients, and caregivers. In addition, the sponsor has
committed to offer appropriate training to sales representatives. To
guard against the inappropriate use of the drug, the RMP also
establishes a multifaceted program for monitoring and surveillance of
abuse. If abuse, misuse, and diversion occur the program includes an
array of interventions.
As part of the RMP, a Medication Guide (FDA-approved patient
information which is required to be dispensed with each prescription)
has been written for patients prescribed Palladone. FDA requires a
Medication Guide only when one or more of the following circumstances
exists: (1) the drug is one for which patient labeling could help
prevent serious adverse effects; (2) the drug is one that has serious
risks of which patients should be made aware because information
concerning the risks could affect patients' decision to use, or continue
to use the drug; and (3) the drug is important to health and patient
adherence to directions for use is crucial to the drug's effectiveness.
In addition, the physician labeling for Palladone contains a “black box”
warning.
FDA is also part of a larger initiative to reduce diversion and abuse
of prescription drugs. On March 1, 2004, the Office of National Drug
Control Policy was joined by the Surgeon General, the DEA Administrator,
and the FDA Commissioner to announce the National Drug Control
Strategy . The strategy emphasized new collaborative efforts at the
federal, state, and local levels to prevent and reduce diversion and
abuse of prescription drugs. This strategy focused on three core
tactics: (1) Business Outreach and Consumer Protection, (2)
Investigation and Enforcement, and (3) Protecting Safe and Effective Use
of Medications. During the approval process for Palladone, FDA
incorporated many of the elements of this strategy as exhibited by
inclusion of the
“black box” warnings on the labeling, the Medication
Guide, and the implementation of a RMP.
In addition to the potential for abuse and addiction, respiratory
depression is the chief potential risk associated with Palladone, if not
properly dosed. Respiratory depression is manifested by a reduced urge
to breathe and a decreased rate of respiration, often referred to as
“shallow” breathing, and can result in severe effects or fatalities. The
risk of respiratory depression is greater in patients not used to taking
opiates, and in elderly or debilitated patients.
Palladone must be swallowed whole because chewing, dissolving, or
crushing the contents of the capsules leads to the rapid absorption of a
potentially fatal dose.
Other common side effects include nausea, vomiting, dry mouth,
dizziness, urinary retention, and constipation.
Palladone is manufactured and distributed by Purdue Pharma L.P.,
located in Stamford, Conn. FDA Clears New Lab Test to Help Screen Newborn
Infants for Congenital Disease
The Food and Drug Administration (FDA) today cleared for marketing a
new laboratory blood test that will help doctors screen newborn infants
for a variety of inherited diseases.
The test is done on blood from newborn heel-stick samples--the same
kind of sample used for state-mandated newborn screening tests. The
blood sample is measured for levels of amino acids and substances
called free carnitine and acylcarnitines.
While small amounts of these substances are found in everyone,
abnormally high amounts, or abnormal patterns, may indicate different
disease states called inborn errors of metabolism. They include, but
are not limited to, phenylketonuria (PKU) and maple syrup urine
disease (MSUD), medium chain Acyl-CoA dehydrogenase deficiency (MCAD),
isovaleric acidemia, homocystinuria and hereditary tyrosinemia.
While each of these individual disorders is relatively rare, as a
group they are fairly common. These diseases can cause developmental
delay, seizures, mental retardation and death.
With early identification, many of the effects of these diseases
can be significantly reduced, with improved long-term outcome and
improved quality of life.
FDA cleared the test based on results of a study of blood samples
taken from more than 200,000 babies. The study was a part of a large
multi-center, epidemiologic study performed by the sponsor. Blood
samples from newborns were tested by current methods and by the new
test, the NeoGram Amino Acids and Acylcarnitines Tandem Mass
Spectrometry Kit.
The NeoGram Amino Acids and Acylcarnitines Tandem Mass Spectrometry
Kit is not a stand-alone test for predicting these kinds of inborn
errors of metabolism. The test provides screening information when
used with clinical evaluation and other tools to determine a newborn
baby’s risk for disorders of amino acid and/or carnitine and/or
acylcarnitine metabolism. Abnormalities are distinguished by elevated
levels or abnormal patterns of amino acids, free carnitine, and
acylcarnitines.
The NeoGram Amino Acids and Acylcarnitines Tandem Mass Spectrometry
Kit is manufactured by PerkinElmer Life and Analytical Sciences, Inc.
of Norton Ohio.
FDA Approves Two Fixed-Dose Combination Drug Products
For the Treatment of HIV-1 Infection
The Food and Drug Administration (FDA) today announced the approvals
of Epzicom (abacavir/lamivudine) and Truvada (tenofovir disoproxil/emtricitabine),
two fixed-dose combination treatments for HIV-1 infection. Control of
HIV/AIDS generally requires simultaneous use of three or more drugs from
different classes. Combination products bring together different
HIV/AIDS drugs in a single medication or co-package and help make
treatment regimens less complicated for patients to follow.
"We gained important scientific knowledge during the development of
these products that will be especially useful in our efforts to speed
the availability of safe and effective fixed-dose combination products
to those who need them in this country and in developing countries..."Simplifying treatment regimens by reducing the number of pills and
times per day patients need to take them provides significant public
health benefits," Dr. Crawford added.
Epzicom and Truvada are indicated for use in combination with other
antiretroviral drug products from different classes such as
non-nucleoside reverse transcriptase inhibitors or protease inhibitors
for the treatment of adults with HIV-1 infection.
Epzicom is a fixed-dose combination of the antiretroviral drugs
abacavir sulfate 600mg and lamivudine 300mg, both of which are approved
individually under the brand names Ziagen (abacavir sulfate) and Epivir
(lamivudine). Epzicomís approval is based on a large well-controlled
clinical study which showed that abacavir dosed once daily had a similar
antiviral effect as abacavir dosed twice daily both in conjunction with
lamivudine and with efaviranz, another antiretroviral drug.
Truvada is a fixed-dose combination of the antiretroviral drugs
tenofovir disoproxil fumarate 300mg and emtricitabine 200mg, both of
which are approved individually under the brand names Viread and Emtriva,
respectively. The approval of Truvada is based on data demonstrating
therapeutic equivalence between the combination product and the
individual products.
FDA completed its review of Epzicom in 10 months and its review of
Truvada in 4 months. GlaxoSmithKline submitted their New Drug
Application (NDA) for Epzicom in October 2003. Gilead Sciences, Inc.,
submitted their New Drug Application (NDA) for Truvada in March 2004.
- FCC
PROPOSED TO PLACE CABLE AND NET PHONES UNDER WIRETAP RULE
The Federal Communications Commission proposed
that Internet-based phone and broadband services to design their
networks so they can be easily wiretapped. This action would assist
the FBI in monitoring the communications of criminals and terrorists.
This would liken these services to phone calls which currently are
under the Communications Assistance for Law Enforcement Act (CALEA).
This law requires “telecommunications” carriers to make their networks
wiretap-friendly. The law will probably also be written to include
walkie-talkie services as well.-InfoJustice
- DOJ
INDICTS SO CALLED NATURAL CARE PRODUCER
United States Attorney Carol C. Lam announced that a
Grand Jury sitting in the Southern District of California returned an
eight-count indictment against San Diego-based corporation Metabolife
International, Inc., and its founder, Michael J. Ellis. The indictment
charges both defendants with six counts of making false, fictitious and
fraudulent representations to the Food and Drug Administration (“FDA”),
and two counts of corruptly endeavoring to influence, obstruct and
impede proceedings concerning the regulation of dietary supplements
containing ephedra being conducted by the FDA, an agency of the
Department of Health and Human Services. Until FDA banned the sale of ephedra in the United States in 2003, Metabolife was one of the largest
retailers of dietary supplements in the United States, based largely on
sales of its ephedra-based product, Metabolife 356.
According to Assistant United States Attorneys
Phillip L.B. Halpern and Kyle W. Hoffman, who are prosecuting the case,
Metabolife and Ellis are charged with falsely representing a number of
different material facts to the FDA in letters dated April 17, 1998 and
February 9, 1999. These representations included false statements by the
Defendants that “Metabolife ha[d] never received one notice from a
consumer that any serious adverse health event has occurred because of
the ingestion of Metabolife 356” and that the company
had a “claims-free history.”
United States Attorney Lam said, "It is never
acceptable for corporations to lie to regulatory agencies, but it is
particularly egregious when those lies threaten the public health."
"One of FDA's highest priorities involves our
responsibility to ensure that information about products we regulate is
truthful and not misleading, because people depend on that information
to make informed choices," said Acting FDA Commissioner Dr. Lester M.
Crawford. "We will pursue to the full extent of the law those who would
seek to mislead consumers by providing false information or impeding
investigations of risky products."
This case is being investigated by the FDA Office
of Criminal Investigations and the IRS Criminal Investigation Division.
United States Attorney Lam stated that the investigation is continuing.
The defendants are scheduled to be arraigned
before Magistrate Judge Louisa Porter in San Diego on Tuesday, July 27,
2004 at 10:30 a.m.
DEFENDANTS Case Number: 03 CR 1088-J
Metabolife International, Inc.
San Diego, CA
Michael J. Ellis
SUMMARY OF CHARGES AND MAXIMUM PENALTIES
Making False Statements to the Food and Drug
Administration in violation of Title 18, United States Code, Section
1001 (Counts 1, 2, 3, 5, 6 and 7)
Maximum penalty is five years in prison and a fine
not to exceed $250,000.
Obstruction of Agency Proceedings in violation of
Title 18, United States Code, Section 1505 (counts 4 and 8)
Maximum penalty is five years in prison and a fine
not to exceed $250,000
PARTICIPATING AGENCIES
Food and Drug Administration, Office of Criminal
Investigation
Internal Revenue Service, Criminal Investigation Division
-
FDA Warns Consumers About Counterfeit Drugs Purchased in Mexico
The Food and Drug Administration (FDA) is
warning the public about counterfeit versions of the drugs Zocor (simvastatin)
and carisoprodol that were recently imported from Mexico by individual
Americans. Tests indicate that the counterfeit Zocor did not contain
any active ingredient and that the counterfeit carisoprodol differed
in potency when compared to the authentic product. Carisoprodol is a
drug used in the treatment of painful musculoskeletal conditions and
Zocor is a cholesterol lowering drug. The counterfeit versions were
reportedly purchased at Mexican border town pharmacies and sold under
the names Zocor, 40/mg, (lot number K9784, expiration date November
2004), and Carisoprodol, 350/mg, (lot number 68348A). Patients who
rely on these counterfeit versions of the drugs could develop serious
health risks (with the counterfeit Zocor) or have insufficient pain
relief (with the counterfeit carisoprodol).
FDA has repeatedly expressed its concern about
the purchase by Americans of drugs from foreign countries. As
demonstrated by this incident, purchasers cannot assume that the
products meet the quality, efficacy, and safety standards of FDA
authorized products or that FDA is assuring the quality, safety, and
efficacy of products purchased from outside the United States.
Medications purchased within the US system for
prescription drugs have undergone rigorous testing and review to
verify their identity, potency, and purity and to ensure that they are
safe and effective for their intended use. In addition, there are
safeguards to help maintain the integrity of the products while in
shipment to pharmacies and prior to dispending to patients.
Anyone who may have recently purchased the above
described versions of Zocor 40/mg and Carisoprodol 350/mg from Mexican
pharmacies should consult with their physician as well as notify their
local FDA field office.
FDA is investigating this matter and working
with the Mexican authorities to ensure that further sale and
importation of these products is halted
FDA ALERTS
CONSUMERS NOT TO FEED INFANTS. CHINESE INFANT FORMULA
The Food and Drug Administration is warning consumers not to feed
their infants infant formula from China because the safety and
nutritional adequacy of infant formula from China is unknown. Recently,
infant formula from China by the name of Guan Wei Yuan was found for
sale in an Asian retail market in New York.
To date, FDA is not aware of any illnesses or injuries associated
with Chinese infant formula, Guan Wei Yuan. However, the analysis of
certain Guan Wei Yuan powdered formulas by the New York State Department
of Agriculture and Markets food laboratory found the formula to contain
less than 1/7 of the federally required minimal amount of protein per
serving, approximately 1/4 the required amount of fat and only minute
amounts of declared calcium and magnesium. There is no guarantee that
this product, as a potential sole source of nutrition, would provide
adequate nutrients for an infant. Consumption by infants, under
conditions of use described on the label and labeling, could result in
outcomes including severe illness or death.
The federal law requires that any infant formula marketed in the U.S.
must be registered with the FDA at least 90 days before marketing.
Manufacturers are required to provide assurances that they are following
good manufacturing practices and quality control procedures and that the
formula will allow infants to thrive. Such assurances have not been
provided for any infant formulas from China. Therefore, the agency is
warning consumers that the safety and nutritional adequacy of infant
formula from China is unknown.
FDA will continue to investigate and work with New York State
Department of Agriculture and Markets and alert other states of the
findings.
Consumers are advised to report any adverse reactions related to
infant formula immediately to your health care provider as well as the
FDA and state
and local agencies.
-
FDA TO PROVIDE
CLEARER INFO TO DRUG SPONSORS CONCERNING REVIEWS OF NEW DRUG
APPLICATIONS
The Food and Drug Administration (FDA) is proposing to change the new
and generic drug review processes by replacing "approvable letters" and
"not approvable letters" with "complete response letters" that provide
companies with specific information about what needs to be done before
their drugs can be approved for marketing. This approach has been used
by FDA for biological drugs for some time and would be formalized for
all drugs by this proposal.
These changes will ensure a single, consistent method of advising
drug manufacturers that FDA review of an application is complete.
"This new approach will provide a clearer and more consistent method
for communicating to new and generic drug applicants about the status of
their applications," said Dr. Lester M. Crawford, Acting Commissioner of
Food and Drugs.
In addition, the proposed rule would amend the provisions on
extending the review cycle for amendments to an unapproved application
and for starting a new cycle after a resubmission in answer to a
"complete response" letter.
Under existing regulations, a resubmission of a new or generic drug
marketing application extends the review period following receipt of an
"approvable" or "not approvable" letter.
Under the new proposal, responses to "complete response" letters for
new drug applications would be classified by what needs to be done to
obtain marketing approval. A "Class 1" resubmission would be defined as
an application resubmitted after receipt of a "complete response" letter
that includes only certain items such as draft or final printed
labeling, safety or stability updates, or other minor clarifying
information. A "Class 1" resubmission would start a new, two-month
review cycle.
A "Class 2" resubmission would be one that would require information
beyond that called for in a "Class 1" resubmission (for instance,
information that would need to be presented at a public advisory
committee meeting). A "Class 2" resubmission would start a new,
six-month review cycle.
The agency's proposal would retain the current "major" and "minor"
terminology for resubmissions of generic drug applications. Under the
proposal, a "major" generic drug marketing application resubmission
would start a new, six-month review cycle. A "minor" generic drug
application resubmission would start a new cycle of from 30 days to a
few months, depending on the issues involved.
These changes to the regulations are proposed to implement the user
fee performance goals referred to in the Prescription Drug User Fee
Amendments of 2002 (known as PDUFA III) that address procedures and
establish target timeframes for reviewing human drug applications.
In conjunction with the Prescription Drug User Fee Act of 1992 (PDUFA),
FDA committed to meet certain goals for reviewing and deciding on human
new drug applications. FDA's drug application review performance goals
were revised with the enactment of the Food and Drug Administration
Modernization Act of 1997 (the user fee provisions of this act are known
as PDUFA II).
FDA's performance goals were further revised in conjunction with the
enactment of PDUFA III, set forth in the Public Health Security and
Bioterrorism Preparedness and Response Act of 2002. Section 502 of PDUFA
III states that user fees will be dedicated to expediting the drug
development process and the process for the review of human drug
applications in accordance with the new performance goals.
WASHINGTON, D.C.
- The Justice Department announced that William C. Murphy, 54, of
Glencoe, Alabama was sentenced today in U.S. District Court to 41 months
in prison, ordered to pay $45,305 in restitution, and was given 3 years
supervised release for selling counterfeit and misbranded pesticides to
municipalities in Alabama and Georgia for mosquito and West Nile Virus
control.
In January,
shortly before his trial was to begin, Mr. Murphy pled guilty to a
twenty-eight count indictment charging him with having manufactured and
sold counterfeit pesticides by using registered brand names that he had
no authority to use in the marketing of chemicals he mixed and packaged
in an Anniston, Alabama warehouse. According to the indictment, Murphy,
operating under the name Sierra Chemical, sold imitations of brand-name
pesticides which bore labels falsely identifying the brand name,
manufacturer, or active ingredients to the following municipalities:
Enterprise, Linden, Alexander City, Brundidge, Jacksonville, Oneonta,
Talladega, Weaver, Cullman, Pell City, Union Springs, Tallassee, and Lee
County, Georgia.
Murphy, who has
been held in prison since his arrest in May, could have received a
maximum fine of $2,000,000 and imprisonment of up to ten years for
violating federal trademark protection laws, and a fine of up to
$100,000 per count and imprisonment of up to one year per count for
violation of federal pesticide control laws.
"This case is an
example of how state and federal agencies can work together effectively
to bring to justice those who violate the environmental laws that both
the state and federal governments have a responsibility to enforce,"
said Thomas L. Sansonetti, Assistant Attorney General of the Justice
Department's Environment and Natural Resources Division. "This
Administration takes seriously its obligation to protect the public
health and the environment. Those individuals and corporations whose
conduct creates such a threat or who knowingly violate environmental
laws will face the kind of prosecution and punishment demonstrated
here."
"The sentence
imposed in this case demonstrates the seriousness of environmental
crimes, and my commitment to protecting the public from those who
perpetrate such crimes," said U.S. Attorney Alice H. Martin.
David McLeod,
Resident Agent in Charge, Environmental Protection Agency said,
"Murphy's sentence should send a clear message to those persons who
think they can get away with undermining the regulatory system that is
intended to ensure the safety and efficacy of the pesticides sold in
this country. It also demonstrates that we take these matters seriously
and will vigorously investigate those who endanger public health."
This case was
investigated cooperatively by Special Agents of the U.S. Environmental
Protection Agency, Criminal Investigative Division and Office of
Inspector General, the Federal Bureau of Investigation, and the Alabama
Department of Agriculture and Industry.
Assistant United
States Attorney Robert O. Posey, Department of Justice Environmental
Crimes Section Senior Trial Attorney Jeremy Korzenik, and Environmental
Protection Agency Region IV Senior Counsel Richard Glaze prosecuted the
case DIETARY CURE
"OVER 650" DISEASES, SEASILVER USA ET AL SIGN FDA DECREE TO STOP SELLING
The Food and Drug Administration (FDA) today
announced that Seasilver USA, Inc., and Americaloe, Inc., of Carlsbad,
California, and their principals, Bela Berkes and Jason Berkes, have
signed a consent decree of permanent injunction in which they agreed to
stop manufacturing and distributing violative products, including
“Seasilver” – a purported cure-all liquid supplement. This action is the
culmination of coordinated efforts by FDA and the Federal Trade
Commission (FTC) to act against the marketing of these violative
products.
“This is yet another example of FDA’s strong
commitment to protect the public from unscrupulous dietary supplement
manufacturers that make unsubstantiated drug claims,” said FDA
Commissioner Mark B. McClellan, M.D., Ph.D.
The consent decree gives FDA the authority to
order the firm to discontinue the marketing of and recall any products
that violate the law in the future. The decree also allows for
liquidated damages for any further violations. The liquidated damages
provision of the consent decree requires the companies and their
principals to pay $1,000.00 for each article distributed in interstate
commerce in violation of the consent decree, the retail value of each
lot manufactured in violation of the consent decree, but not distributed
in interstate commerce, and $10,000.00 per day, per violation for any
other violations of the consent decree. The consent decree was signed on
March 8, 2004, by United States District Judge William Q. Hayes in San
Diego, Calif.
This consent decree follows a coordinated effort
in June 2003 between the Federal Trade Commission (FTC) and the FDA
against Seasilver U.S.A., Inc., and Americaloe, Inc., their owners, and
two of the companies' principal distributors. On June 16, 2003, at FDA’s
request, U.S. Marshals seized 132,480 bottles of Seasilver, worth nearly
$5.3 million, from Seasilver USA’s San Diego headquarters.
The Government’s complaint alleges that, although
Seasilver USA markets Seasilver as a dietary supplement, the companies
promote it on the Internet and in marketing materials sent with the
product as a treatment for “over 650” diseases including, for example,
cancer, heart disease, stroke, diabetes, hepatitis, arthritis,
depression and other diseases. These claims cause Seasilver to be an
unapproved new drug under the Federal Food, Drug, and Cosmetic Act (FD&C
Act). Such claims also cause Seasilver to be misbranded under the FD&C
Act because it lacks adequate directions for use.
Seasilver’s labeling also contains claims such as
“cleanses your vital organs” and “oxygenates your body’s cells.” These
claims show that Seasilver is intended to affect the structure or
function of the body. Because the claims are unsubstantiated, Seasilver
is misbranded under the FD&C Act.
The FTC, which regulates dietary supplement
advertising, alleges, in part, that the defendants promoted Seasilver
through false claims that it was clinically proven to treat or cure 650
diseases, including cancer and AIDS. Under a settlement with the FTC,
entered on March 4, 2004, the Seasilver defendants and the individual
distributors agreed to pay $4.5 million in consumer redress. In
addition, the FTC settlements also bar defendants from making any false
or misleading claims about the benefits of any food, drug, or dietary
supplement.
"The claims for Seasilver threatened consumers’
health by encouraging delays and replacements for proven treatments,"
said Howard Beales, Director of the FTC's Bureau of Consumer Protection.
"The FTC and FDA are committed to taking aggressive action against false
and unsubstantiated claims in the dietary supplement market. Products
touted as cure-alls almost always cure nothing.”
As a result of FDA’s consent decree, Seasilver
U.S.A. and Americaloe, Inc., will destroy the seized products at their
expense under the supervision of a Department of Health and Human
Services representative within 60 days of posting bond.
 GLENDALE MAN INDICTED
FOR TRAFFICKING IN COUNTERFEIT VIAGRA TABLETS;
"YOU JUST CANNOT MAKE THIS STUFF UP-little
guy"
GLENDALE MAN INDICTED
FOR TRAFFICKING IN COUNTERFEIT VIAGRA TABLETS;
"YOU JUST CANNOT MAKE THIS STUFF UP-little
guy"
U.S. Department of Justice,
United States Attorney's Office,
Central District of California (Los Angeles)
- NEWS RELEASE
-
A federal grand jury in Los Angeles today indicted
a Glendale man on charges of trafficking in counterfeit Viagra tablets
that were manufactured in the People's Republic of China.
Khoa Twan Do, also known as Chris Do, 31, was
named in a three-count indictment returned this afternoon by the grand
jury.
The indictment alleges that Do conspired with a
manufacturer in Beijing to import at least 40,000 counterfeit Viagra
tablets into the United States. Do arranged to have the bogus Viagra
tablets shipped to his business, Health Plus in Glendale, from which he
would resell the fake goods.
The indictment alleges that Do told his Beijing
supplier that the counterfeit tablets needed to "look like the real
thing" because "I can find many customers who want the real thing."
"This is another example of the hazards presented
by importation of counterfeit foreign drugs into North America," said
FDA Commissioner Mark B. McClellan, M.D., Ph.D. "It's a form of the
medical black market that endangers the public health and cannot and
will not be tolerated."
The indictment alleges one count of conspiracy,
one count of trafficking in counterfeit goods and one count of selling a
counterfeit drug. The three counts in the indictment carry a maximum
possible penalty of 18 years in federal prison and a fine of more than
$2 million.
An indictment contains allegations that a
defendant has committed a crime. Every defendant is presumed innocent
until and unless proven guilty.
Do will be summoned to appear for an arraignment
in United States District Court in Los Angeles on January 26.
This investigation was conducted by the United
States Bureau of Immigration and Customs Enforcement, and the Food and
Drug Administration's Office of Criminal Investigation.
John M. Taylor, the FDA's Associate Commissioner
for Regulatory Affairs, stated: "This indictment is a good demonstration
of inter-agency cooperation at its best. FDA will continue to work
closely with its law enforcement colleagues as part of its absolute
commitment to aggressive enforcement of the laws that protect patients
from unsafe medications."
January 9, 2004
CONTACT: The Honorable Assistant United
States Attorney John Owens (213) 894-3315...
-
HAPPY NEW YEARS AMERICA
 The American
Academy For Justice Through Science wishes all Americans a safer, more
prosperous, healthier and happier 2004. God Bless America.-"little
guy"- The American
Academy For Justice Through Science wishes all Americans a safer, more
prosperous, healthier and happier 2004. God Bless America.-"little
guy"- -
FDA
COUNTERFEIT POLYPROPYLENE HERNIA REPAIR MESH ALERT;
"YOU JUST CANT MAKE THIS STUFF UP"-"little
guy cfe"
The Food and Drug Administration (FDA) today alerted healthcare
professionals to a counterfeit polypropylene mesh product labeled as
PROLENE polypropylene mesh. The product is a non-absorbable mesh used in
hernia repair and other surgery. The authentic PROLENE mesh is
manufactured by Ethicon, Inc. Ethicon issued an alert to healthcare
professionals about the counterfeit product on October 28.
Preliminary testing of the counterfeit PROLENE by FDA indicates that
some samples are not sterile, although at this time FDA is not aware of
a significant increase in the number of infections related to use of the
counterfeit product. Additional preliminary testing indicates that the
counterfeit product has a molecular structure similar to other
polypropylene mesh products currently on the market. FDA is continuing
to test the material.
FDA is continuing to investigate whether the counterfeit product is
still being marketed. In the meantime, FDA recommends that healthcare
professionals carefully examine all polypropylene mesh products and not
use any suspected of being counterfeit. If they believe the counterfeit
product may have been implanted in patients, they should continue to
monitor the patients as they would any patient with a polypropylene mesh
implant. Although FDA has not had reports of excess infections with the
counterfeit product, the agency continues to be concerned about
sterility.
The counterfeit mesh is labeled with lot numbers RBE609 (expiration
date 1/07) and RJJ130 (expiration date 7/07). It can be further
identified by one of the following:
- A packaging seal that does not tear open smoothly;
- An additional small seal on top corner edges of the package;
- A fabric end that is jagged or not cleanly cut on the 3” side; and
- An Ethicon logo in a thicker than usual typeface.
In a Public Health Notification issued today, FDA encouraged the
medical community to report adverse events related to the counterfeit
mesh to the FDA through procedures established by their medical facility
or through MedWatch, the FDA’s voluntary reporting program.
The “Public Health Notification on Counterfeit Polypropylene Mesh” is
available at
http://www.fda.gov/cdrh/safety/121903.html.
Ethicon also manufactures PROLENE sutures, which are not the subject
of this alert. -
CONGRATULATIONS PLANET EARTH; "SADDAM IS OVER"
Some say that the age of chivalry is
past, that the spirit of romance is dead. The age of chivalry is never
past, so long as there is a wrong left unredressed on earth."
Charles
Kingsley,
Vol., II,
Ch 28: "A
good conscience is a continual Christmas." Ben Franklin
Rarely in mankind's
experiential existence, can history report a time when the entire world
benefited by the capture of a criminal. This criminal, this
Saddam, held captive the hearts, the minds, the earth souls and of
freedom of the Iraqi peoples in the past and in the present. This new
"bastion of humanity", this new Iraq, can now attempt to contribute to the
human experience in a positive way. With a free Iraq, if possible,
this will facilitate a free world. And further demonstrate that no
criminal can escape the law for the "Wheel of Justice Turns Slowly Yet
Finely".
In some ways it is sad
that the world will celebrate at the capture of a very sick human being.
Yet, with the world still where we
are relative to human progress, Saddams' capture symbolizes the
greatness of good.
The strength of love over hate.
The enormity of the human spirit to rise above evil, and bring all that
is good, such as "freedom" to all peoples no matter their color, creed
or race. Last evening, Yankee
Doodle
Dandies
in the form of US Special forces
working with Army Infantry, prove once again, that when "Uncle
Sam" wants
you, you go. Sam
wanted Saddam, we went, and Saddam now teaches the world that good does
triumph over evil, albeit it is sometimes a hard example to illustrate.
Congratulations to all Americans, to all Iraqis, and to all peoples.
We as citizens earth, may yet prove someday, it will be a free world, a
safe world, a caring world and a "God Loving" world. -"little guy"-12-14-2003
-
FDA AND CBP POLICY
ON
FOOD IMPORTS UNDER
THE BIOTERRORISM ACT
This press release replaces an earlier version.
The United States Food and Drug Administration (FDA) and the U.S.
Bureau of Customs and Border Protection (CBP) today issued a
compliance policy
guide that describes their strategy for maintaining an uninterrupted
flow of food imports while improving their safety in accordance with the
Public Health Security and Bioterrorism Preparedness and Response Act of
2002 (Bioterrorism Act).
The policy guide deals with the enforcement of the Bioterrorism Act's
requirement, which becomes effective on December 12, 2003, that FDA
receive a prior notification of all human and animal food, drinks and
dietary supplements imported or offered for import to the U.S. Another
requirement of the Bioterrorism Act mandates that all facilities that
manufacture, process, pack or hold food for consumption in the U.S. be
registered with FDA. This registration requirement for foreign
facilities will be primarily enforced through the prior notice
provision.
In October, FDA and CBP jointly published an interim final rule that
specified that, among other requirements, the prior notice must be
received by FDA between two and eight hours -- depending on the mode of
transportation -- before each shipment's arrival at the U.S. border. The
prior notice interim final rule also covers food packages mailed or
brought to the U.S. by individuals from abroad.
As the rule becomes effective, FDA and CBP expect a "good faith"
effort at compliance. The policy guide issued today makes clear that
during the next 8 months, the two agencies will primarily rely on
educating the affected firms and individuals. During this period, the
agencies will utilize communication and education initiatives,
escalating imposition of civil monetary penalities, and ultimately
refusal of shipments. This phase-in period will end on August 12, 2004.
As always, both agencies will continue to ensure that imported products
are safe for human or animal consumption. Regarding food mailed, brought
or accompanied to the U.S. by individuals for non-personal use, FDA and
CBP generally will continue their education efforts and will not refuse
its admission before August 12, 2004 because of inadequate or lacking
prior notice.
"Our intention all along has been to implement the Bioterrorism Act
in a way that would protect consumers without obstructing the food
imports, on which we depend for 20 percent of all fresh produce and up
to 60 percent of all the seafood consumed in the U.S.," said FDA
Commissioner Mark B. McClellan, M.D., Ph.D. "The goal of the transition
policy is to provide complete clarity and education about the new import
requirements, and achieve a higher level of U.S. food security without
disrupting trade. I am satisfied that this policy guide presents a
realistic strategy for facilitating the flow of this essential commerce,
as well as holiday food packages, while countering the threat of
terrorism."
U.S. Customs and Border Protection Commissioner Robert C. Bonner
said, "We at the CBP for decades have worked closely with the FDA in
ensuring the safety and security of imported foods, especially
perishables, that reach our dinner tables every day. The Bioterrorism
Act provides us with yet another highly effective tool to safeguard
America's food supply from the terrorist threat."
FDA and CBP personnel have already begun an extensive campaign to
educate with written material, briefings, and seminars other government
officials, domestic and foreign food importers, brokers, transporters,
and other affected industry representatives on compliance with the
Bioterrorism Act. In addition, during the 8-month transitional period,
the two agencies plan to take the following steps:
- Gather data to track compliance with the prior notice requirements
and to determine how to best use FDA's and CBP's resources to educate
industry and the public to achieve full compliance with the
Bioterrorism Act.
- Provide industry and the public with summary information about the
level of compliance with the prior notice rules, including data on the
types of errors in submitted prior notices.
- Post the summary information on FDA's website at
www.fda.gov.
- Use the data and summary information to assist the industry and
the public in improving the submission of prior notice.
During the phase-in period, FDA and CBP will generally use civil
monetary penalties and refusals only in response to repetitive, flagrant
and other serious violations.
The policy guide clarifies, however, that FDA and CBP will continue
their surveillance of food imports to ensure they are safe, wholesome,
and that they comply with other U.S. requirements. The transitional
policy announced today does not affect FDA’s or CBP's ability to
initiate other actions to protect U.S. consumers. If FDA decides during
and after the transition period not to refuse an imported article of
food under the provisions of the Bioterrorism Act, such decision will
have no bearing on whether the article is admissible on other grounds.
Thus, for food that is imported or offered for imports, FDA will
continue to carry out such routine food safety- and security-focused
reviews, investigations, and enforcement actions as may be necessary.
From December 12, 2003 on, the enforcement of the Bioterrorism Act will
be carried out, on a round-the-clock, 7 days a week basis, by hundreds
of FDA and CBP employees.
-
FDA ADIVISORY ON METHYLMERCURY
The Food and Drug Administration’s (FDA) Food Advisory Committee (FAC)
will meet on December 10-11, 2003 to receive an update regarding the
recommendations made during the July 2002 FAC regarding fish
consumption and methylmercury. The revisions have resulted in the
first unified FDA and EPA revised advisory concerning all fish and
shellfish consumption for populations at risk from exposure to high
mercury levels: pregnant women, nursing mothers, women who may become
pregnant, and young children. In addition, the FAC will review reports
from subcommittees: Infant Formula, Contaminants and Natural
Toxicants, Dietary Supplements, Additives and Ingredients and Food
Biotechnology. The meeting will be held at the Hotel Washington,
Pennsylvania Avenue at 15th Street, Washington, D.C. 20004-1009.
In July 2002, FDA’s Food Advisory Committee met and made several
recommendations to FDA on how to revise its consumer advisory on
methylmercury in fish with special concern for pregnant women, nursing
mothers, women who may become pregnant, and young children. One of
these was for FDA and EPA to coordinate mercury advisories on
commercial fish and recreational fish. Additionally, they recommended
that the issue of tuna consumption be addressed.
FDA and EPA have been working diligently toward the goal of
updating the consumer advisory in response to the recommendations from
the Food Advisory Committee. This work has included: conducting
ongoing interagency meetings; conducting field assignments which
provided additional testing of methylmercury in fish for which there
were low sample sizes; sampling 300 cans of tuna; undertaking exposure
assessments using these new data; and testing the revised advisory
with focus groups. As part of the meeting, FDA is seeking
recommendations or concurrence from the committee before finalizing a
joint FDA and EPA revised advisory concerning fish and shellfish
consumption. The revised advisory now contains information concerning
consumption of all fish, including both commercial fish and locally
caught fish. Following the Committee’s concurrence, FDA will initiate
an outreach and educational program early in 2004 for at-risk
populations.
This advisory is directed to pregnant women, nursing mothers, women
who may become pregnant, and parents of young children. This is
because the nervous system of the developing fetus and of young
children is most at risk from high methylmercury levels in fish.
- PRESIDENT BUSH SIGNS
IMPORTANT PEDIATRIC LEGISLATION
.
HE BELIEVES OUR CHILDREN ARE THE FUTURE!
President Bush today signed important new legislation that will
enable the United States Food and Drug Administration to improve the quality of health
care for our children.
USFDA has worked diligently to use its available authorities and
resources to give pediatricians and parents the solid information they
need to treat children who are ill. These programs, which include
financial incentives and new funding to conduct needed pediatric
studies, have helped develop needed evidence on the effects of medicines
in children. But in some cases needed studies have not been done. FDA's
most recent attempt to require pediatric studies failed when the U.S.
District Court for the District of Columbia held in October 2002, that
our agency lacked sufficient statutory authority.
When it goes into effect today, the Pediatric Research Equity Act of
2003 will allow FDA to close the knowledge gap when it comes to treating
children. FDA will now have clear authority to require pediatric studies
of drugs when other approaches are not sufficient to ensure that drugs
are safe and effective for children.
Prescription drugs can do more than ever to cure diseases, including
illnesses in children. But it is not good medicine to assume that
children can be treated like little adults. Parents and health
professionals deserve confidence that medicines used to treat children
are safe and effective. USFDA will use this important new law to require
pediatric studies, when necessary, to give parents and doctors the
confidence they deserve.12-07-2003
-
FTC
WORKING WITH YOUR USFDA
In response to a request for public comment by the U.S. Food and Drug
Administration (FDA), the staff of the Federal Trade Commission filed
a comment on December 1, 2003 regarding direct-to-consumer (DTC)
advertising of prescription pharmaceuticals. The staff’s response
analyzes the overall economic effects of such advertising and provides
the FDA with a number of suggestions about how its regulatory scheme
for DTC advertising could be modified to communicate information to
consumers in an easy to understand and accessible way.
According to the staff’s comment, which can be
found as a link to this press release on the FTC’s Web site,
“Empirical evidence suggests that the FDA’s current approach to
regulating DTC advertising generally benefits consumers.” Survey
evidence suggests, according to the staff, that “DTC ads have provided
consumers with useful information about the drug options open to
them,” and this has “empowered consumers to interact with physicians
more effectively.” The comment further states that the available
evidence does not support concerns that DTC advertising has increased
the sale of inappropriate drugs or led to increased drug prices.
Analysis of DTC Advertising
Regulations
The staff comment also makes the following
suggestions regarding how the FDA’s DTC advertising regulatory scheme
could be modified to communicate truthful, non-misleading information
in a way that is easier for consumers to understand and use:
- The brief summary requirement for broadcast ads – a major
statement of drug risks along with adequate provision for more
complete risk information – should be retained, but modified.
- The brief summary requirement for
broadcast ads should be modified so that consumers would be directed
to a more useful source of risk information than the labeling the
FDA approved for the product as part of its drug approval process,
such as FDA-approved patient labeling or other risk information that
has been specifically designed for consumers.
- The brief summary requirement for print
ads – that complete risk information (such as the labeling that the
FDA approved for the product as part of its drug approval process)
be included in the ad – should be made consistent with the brief
summary requirement for broadcast ads.
- The fair balance requirement for DTC ads
should prohibit only ads that convey a deceptive impression of the
risk and benefits from the overall presentation of information,
rather than those that fail to achieve a mechanistic balance between
risk and benefit information.
- Pharmaceutical manufacturers should be
permitted to make truthful, non-misleading price comparisons and
other types of relative cost claims.
- The FDA should apply the same standards
for endorsements and testimonials in DTC ads for prescription drugs
as the FTC applies through its Guides Concerning the Use of
Endorsements and Testimonials in Advertising to endorsements and
testimonials for other products, including over-the-counter (OTC)
drugs.
- Internet advertising should be treated
consistently with DTC ads in other media, and it would be beneficial
if the FDA were to issue a guidance document addressing DTC ads
available on the Internet.
In concluding its comment, the FTC staff writes,
“DTC advertising can play an important role in providing information
about prescription drugs that may spur consumers to seek help for a
previously untreated condition, encourage them to talk with a doctor
about a new drug, or otherwise take a more proactive role in minding
their health. We therefore encourage the FDA to examine ways to
facilitate the flow of truthful, non-misleading information in DTC
advertising in a manner that is easy for consumers to understand and
access.”
The Commission vote authorizing staff to issue the
comment in response to the FDA’s request was 5-0.
NOTE: The views expressed in the letter are those
of the staff of the FTC’s Bureaus of Consumer Protection and Economics
and the Office of Policy Planning, and do not necessarily represent
those of the Commission or any individual Commissioner.
-
FBI HAS NEW WEB PAGE AGAINST SCAMS, SCHEMES, SHAMS, CONS, HUCKSTERISM,
RACKETS, HOAXES, WASTE,
FRAUD AND ABUSE
As of October 4th, 2003 your FBI asks,
"Want
to know more about what the FBI is doing, big picture, to protect you
and your family against fraud? Everything from corporate greedsters to
financing and insurance con men? From criminal telemarketers to medical
scams?
You may not
realize that over one-third of FBI convictions and pre-trial
diversions last year-over 6,000!-fell in the area of white collar
crimes".
-
TEXAS BASED
WEB SCAMMERS
BUSTED. MUST PAY REDRESS
FOR DECEPTIVELY GUARANTEEING CONSUMERS CREDIT CARDS
Texas-based defendants who engaged in a scam in
which they e-mailed consumers promising to provide them with a credit
card agreed to pay $815,000 in consumer redress to settle Federal Trade
Commission charges. The defendants, ClickForMail.com, Inc., doing
business as AllPreApproved.com, and Harvey B. Vaughn, III, were part of
the FTC’s Southwest Netforce sweep that targeted Internet scammers and
deceptive spammers. The FTC alleged that the defendants sent spam e-mail
telling consumers they were approved and guaranteed to receive major,
unsecured credit cards with credit limits up to $5,000 for an advance
fee of $49.95. In addition to paying redress, the settlement prohibits
the defendants from making any false claims to consumers in the future.
In its complaint, filed in May 2003, the FTC alleged
that the defendants sent spam e-mail telling consumers that they were
guaranteed to receive a major, unsecured credit card with a high credit
limit. Interested consumers then “clicked through” to the defendants’
Web site where they allegedly learned that they were required to pay a
$49.95 advance fee to be debited from their checking account before they
could get the card. According to the FTC, however, consumers who paid
the fee did not receive the promised card. Instead, they allegedly
received access to a set of hyperlinks to companies where consumers
could apply for credit cards, and even then those were generally for
secured credit cards, stored-value cards, or catalog charge cards. The
FTC’s complaint alleged that the defendants falsely claimed that: (1)
consumers who met minimum qualifying criteria and paid a $49.95 fee
would receive unsecured major credit cards; and (2) that the defendants
had special arrangements with banks or financial institutions to issue
to its customers unsecured major credit cards.
The proposed settlement announced today prohibits
the defendants from making false claims that they:
- will provide or arrange for consumers to receive major credit
cards;
- have arrangements with banks or financial
institutions to offer credit to consumers; or
- will provide consumers with any
credit-related products, programs, or services.
The settlement also prohibits the defendants from:
(1) misrepresenting any material fact prior to a consumer’s purchase of
any products, programs, or services; (2) assisting others who engage in
any activity that may violate the order; and (3) selling their customer
lists. In addition to the defendants paying redress, the settlement
contains an avalanche clause that requires the defendants to pay $3.6
million if the court finds that they materially misrepresented their
financial status to the Commission.
Finally, the settlement contains various
recordkeeping requirements to assist the FTC in monitoring the
defendants’ compliance.
The Commission vote authorizing staff to file the
stipulated permanent injunction and final judgment order was 5-0. It was
filed in the U.S. District Court for the Northern District of Illinois,
Eastern Division, on October 2, 2003, and was approved by the Court the
same day.
-
FEDERAL AGENCIES
PUBLISH CONSUMER BROCHURE ON PREDATORY LENDING PRACTICES
The federal Interagency Task Force on Fair Lending has published a
new brochure that alerts consumers to potential borrowing pitfalls,
including high-cost home loans, and provides tips for getting the best
financing deal possible. The brochure, Putting Your Home on the Loan
Line Is Risky Business, warns that regardless of whether a home
equity loan is for a home repair, bill consolidation or some other
purpose, it is important to shop around.
Borrowing
from an unscrupulous lender, especially one that
offers a high-cost loan using the home as security, could result in the
loss of the borrower's home and their money. Before signing the
credit contract, consumers are encourage to
- Think
about their financing options
- Do their homework
- Think twice before they sign a loan contract
- Know that they have rights under the law
The members of the Interagency Task Force are the Department of
Housing and Urban Development, Department of Justice, Federal Deposit
Insurance Corporation, Federal Housing Finance Board, Federal Reserve
Board, Federal Trade Commission, National Credit Union Administration,
Office of the Comptroller of the Currency, Office of Federal Housing
Enterprise Oversight, and Office of Thrift Supervision
For a copy of the complete brochure simply click
or contact Justice as listed below:
Department of Justice: The Department's web site at
http://www.usdoj.gov or contact the U.S. Department of Justice,
Civil Rights Division, 950 Pennsylvania Ave., N.W., Housing and Civil
Enforcement Section, NWB, Washington, D.C. 20530; (202) 514-1116.
-
FDA PUBLIC MEETING ON
OBESITY
-
Date and Time: October 23, 2003 from 9:00 a.m. to 5:00 p.m.
Place: Warren Grant Magnuson Clinical Center, Masur
Auditorium, (Bldg. 10) National Institutes of Health, 9000 Rockville
Pike, Bethesda, Md.
Register by October 17, 2003
The Food and Drug Administration will convene a public meeting to
discuss issues within FDA’s jurisdiction related to obesity and
nutrition. The purpose of the meeting is to discuss FDA’s role and
responsibility in addressing the public health problem of obesity,
promoting better consumer dietary and lifestyle choices that have the
potential to improve the health and well-being of Americans, and how
best to build a framework for messages to consumers about reducing
obesity and achieving better nutrition.
The public meeting will address the following questions:
- What is the available evidence on the effectiveness of various
education campaigns to reduce obesity?
- What are the top priorities for nutrition research to reduce
obesity in children?
- What is the available evidence that FDA can look to in order to
guide rational, effective public efforts to prevent and treat obesity
by behavioral or medical interventions, or combinations of both?
- Are there changes needed to food labeling that could result in the
development of healthier, lower calorie foods by industry and the
selection of healthier, lower calorie foods by consumers?
- What opportunities exist for the development of healthier
foods/diets and what research might best support the development of
healthier foods?
- Based on the scientific foundation available today, what are the
most important things that FDA could do that would make a significant
difference in efforts to address the problem of overweight and
obesity?
The Federal Register Notice is available at
http://www.fda.gov/oc/opacom/hottopics/obesity.html
FTC Alleges "Ab Force"
Belt Won't Provide Rock-Hard Abs
Telebrands Corp., TV Savings LLC, and their owner,
Ajit Khubani, have been charged by the Federal Trade Commission with
making the same type of false claims in the marketing and sale of their
"Ab Force" electronic muscle stimulation (EMS) belt as those the FTC
targeted in "Project ABSurd." The FTC alleges in an administrative
complaint announced today that the respondents, through their
advertisements and promotional materials for the Ab Force belt, falsely
claimed that the belt causes loss of weight, inches, and fat; causes
well-defined abdominal muscles; and is an effective alternative to
regular exercise.
In May 2002, as part of "Project ABSurd," the FTC
challenged claims made by the marketers of three widely advertised EMS
belts - the Ab Tronic, AB Energizer, and Fast Abs. The Commission
alleged that the marketers of those products falsely advertised that
users would get "six pack" or "washboard" abs without exercise. In July
2003, the FTC announced a settlement of over $5 million resolving the
Fast Abs litigation. The Commission also announced that the U.S.
district court in Nevada granted the FTC's motion for partial summary
judgment against five of the seven Ab Tronic defendants, holding them
liable for $83 million in redress. The AB Energizer case still is
pending.
"There is no 'free ride' on misleading advertising,"
said Howard Beales, Director of the FTC's Bureau of Consumer Protection.
"If you purposely evoke the false claims made for a similar product,
then your ads also are deceptive. And you should expect to hear from the
FTC."
The FTC's complaint, filed before an administrative
law judge, alleges that the New Jersey-based respondents violated the
FTC Act by representing that Ab Force could produce the same results
touted in the deceptive infomercials for Ab Tronic, AB Energizer, and
Fast Abs.
Those infomercials essentially claimed that users
could achieve weight loss, fat loss, and inch loss, get well-developed
abs, and obtain results that were equivalent to volitional exercise. The
Ab Force ads show well-muscled, bare-chested men and lean, shapely women
wearing Ab Force belts and purportedly experiencing abdominal
contractions. The ads expressly referred to "those fantastic electronic
ab belt infomercials on TV" that the announcer is "sure" the viewer has
seen. According to the FTC's complaint, the Ab Force ads, including
through references to the prior ab infomercials, falsely claimed that:
- Ab Force causes loss of weight, inches, or fat;
- Ab Force causes well-defined abdominal muscles;
and
- Use of Ab Force is an effective alternative to
regular exercise.
Previous FTC Actions
The FTC has taken four previous actions against Ajit
Khubani and Telebrands. In 1990 and 1996, the Commission obtained
consent judgments prohibiting Khubani and his corporations from
violating the Mail or Telephone Order Merchandise Rule (Mail Order Rule)
and requiring them to pay penalties of $35,000 (1990) and $95,000
(1996). In 1999, the FTC modified the existing 1996 consent judgment
with the defendants and obtained penalties of $800,000 to resolve
alleged violations of the Mail Order Rule. In addition, in 1996, the FTC
obtained an administrative order prohibiting Khubani and Telebrands from
violating the FTC Act in connection with the marketing of television
antennas and hearing aids.
In an administrative trial, the FTC will seek to
prohibit Telebrands, TV Savings, and Khubani from making any
misrepresentations about Ab Force or any other EMS device. The FTC also
will seek to prohibit them from making any unsubstantiated
representations about weight, inch, or fat loss, muscle definition, or
the health benefits, safety, or efficacy of Ab Force or any EMS device,
or any food, drug, dietary supplement, device, or any other product,
service, or program.
In addition, as set forth in the notice order, the
FTC is seeking to require Khubani to obtain a $1 million performance
bond before engaging in any manufacturing, labeling, advertising,
promotion, offering for sale, sale, or distribution of any device. The
notice order also includes various reporting requirements to assist the
FTC in monitoring the respondents' compliance with its provisions.
Finally, the notice order notes that the Commission may seek redress for
consumers who purchased the Ab Force.
The Commission vote to issue the administrative
complaint and notice order was 5-0.
NOTE: The Commission issues s a
complaint when it has "reason to believe" that the law has been or is
being violated, and it appears to the Commission that a proceeding is in
the public interest. The complaint is not a finding or ruling
that the respondents have actually violated the law. Such action marks
the beginning of a proceeding in which the allegations will be ruled
upon after a formal hearing.
-
USFDA
APPROVES
Stair-Climbing Wheelchair
The Food and Drug Administration (FDA) today approved a
battery-powered wheelchair that relies on a computerized system of
sensors, gyroscopes and electric motors to allow indoor and outdoor use
on stairs, as well as on level and uneven surfaces.
FDA expedited review of the product, called the INDEPENDENCE iBOT
3000 Mobility System, because it represents a breakthrough technology
with the potential to benefit people with disabilities. An estimated 2
million people in the United States use wheelchairs.
"This wheelchair represents a breakthrough in wheelchair technology,"
said FDA Commissioner Mark B. McClellan, M.D., Ph.D. "It can help
improve the quality of life of many people who use wheelchairs by
enabling them to manage stairs, reach high shelves and hold eye-level
conversations. Its approval is emblematic of FDA’s commitment to help
innovative medical technologies reach patients promptly."
The user can push a button to command the wheelchair to operate in
several different ways. It can be easily converted from a standard chair
with four wheels contacting the ground to an elevated chair balanced on
only two wheels. This is done when the user wants to reach high objects
or wants to be at eye level for conversation. Four-wheel drive enables
the user to traverse rough terrain, travel over gravel or sand, go up
slopes, and climb 4-inch curbs. For use on stairs, there are two sets of
drive wheels that rotate up and over each other to climb up or down, one
step at a time. Because of its unique balancing mechanism, the
wheelchair remains stable and the seat stays level during all these
maneuvers.
To climb up stairs, the occupant backs up to the first step and holds
onto the stair railing. Then he shifts his weight over the rear wheels,
causing the chair to begin rotation of the front wheels up over the rear
wheels and then down onto the first step. As the user shifts his weight
backward and forward, the chair senses this and adjusts the wheel
position to keep his center of gravity under the wheels. The chair
ascends stairs backward and descends forward (the user always faces down
the stairs).
To reach high shelves or hold eye-level conversations with people who
are standing, the occupant shifts his weight over the back wheels so
that the iBOT lifts one pair of wheels off the ground and balances on
the remaining pair of wheels. The user then presses a button to lift the
seat to a higher position.
People must weigh no more than 250 pounds and must have the use of at
least one arm to operate the chair. They also must have good judgment
skills to discern which obstacles, slopes, and stairs to avoid in order
to prevent serious falls. Users must be capable of some exertion when
climbing stairs in the wheelchair by themselves. However, for users who
cannot tolerate such exertion, there is a feature that allows someone
else to hold onto and tilt the chair’s back to cause it to climb up or
down stairs.
Physicians and other health professionals must undergo special
training to prescribe the iBOT. The chair must be calibrated to the
patient’s weight, and patients have to be trained in its use and pass
physical, cognitive and perception tests to prove they can operate it
safely.
FDA approved the wheelchair based on a review of extensive bench
testing of the product conducted by the manufacturer, Independence
Technology (a Johnson & Johnson company), of Warren, N.J., and on a
clinical study of its safety and effectiveness. Approval was also based
on the recommendation of the Orthopedic and Rehabilitation Devices Panel
of FDA’s Medical Devices Advisory Committee.
The firm performed a wide range of tests on the chair, including
mechanical, electrical, performance, environmental and software testing.
In the pivotal clinical study, 18 patients—mostly people with spinal
cord injury-- were trained to use the iBOT and test-drove it for two
weeks to allow researchers to compare maneuverability, falls and other
problems to those encountered with their regular wheelchairs. They also
tested it going up hills, over bumpy sidewalks, crossing curbs, reaching
shelves and climbing stairs. Twelve patients could climb up and down
stairs alone with the iBOT. The other six patients used an assistant.
When these same 18 patients used their regular wheelchairs, one patient
could "bump" down stairs, but no one could go up even one step.
During the pivotal study, three patients fell out of the iBOT and two
fell out of their own wheelchairs. None of the falls occurred on stairs.
Two patients experienced bruises while using the iBOT.
As a condition for approval, the manufacturer has agreed to provide
periodic reports to the FDA to document the chair’s usage, functioning
and any patient injuries.
-
FDA APPROVES LICENSE OF NEW RECOMBINANT
ANTI-HEMOPHILIC FACTOR
-
FDA today licensed a new recombinant DNA-derived clotting factor to
treat people with hemophilia A. This new antihemophilic human factor
VIII product is the first one produced without using additives derived
from human or animal blood in the manufacturing process.
This advancement provides added reassurance against any theoretical
infectious risks that may arise from the use of blood-derived additives
in the manufacturing of factor VIII.
The new product, called ADVATE Antihemophilic Factor (Recombinant),
Plasma/Albumin-Free Method (rAHF-PFM), is approved to prevent and
control bleeding episodes or to prepare persons with hemophilia for
surgery. It is produced by genetically engineered Chinese hamster ovary
cells that have been altered to produce factor VIII.
A number of human factor VIII products have been approved to treat
hemophilia A, an inherited disorder in which the blood clotting protein
factor VIII is deficient or abnormal. Affected persons are unable to
form blood clots normally and therefore risk serious and
life-threatening bleeding episodes. Replacement therapy with any of the
factor VIII products, which requires intravenous administration,
corrects the defect only temporarily. For this reason, factor VIII
products frequently must be given several times a week, or more often,
to prevent or treat bleeding episodes.
Current factor VIII products (both plasma-derived and recombinant)
are considered very safe as a result of many technological advances in
the last two decades. These include viral inactivation and removal steps
in manufacturing that are believed to effectively prevent transmission
of hepatitis B, hepatitis C or HIV from plasma-derived products. These
same procedures are considered effective to minimize any infectious
risks from products made by DNA technology, which uses living cells.
None of these products has transmitted HIV, hepatitis B or hepatitis C
since 1987.
The first recombinant antihemophilic factor was approved in 1992.
However, up until now, all recombinant factor VIII products still were
made with the use of blood-derived additives of human or animal origin,
such as albumin. These additives were needed to keep the cells viable so
they could make the factor VIII protein. In this new product non-human
and non-animal materials replaced these additives.
-
HO, HUM. FRAUD, A DAILY THEFT
OF THE TRUST OF A NATIONS CONSUMERS. HO, HUM. HUCKSTERS FLOURISH
UNDER SEC:
ACM Income Inc.'s (ACG)
investment manager, Alliance Capital Management
underwent unusual trading which took
place this month.
Edmund Bergan, chief counsel at Alliance, advised
during a recent conference call "The
activity on July 8 did our shareholders a disservice," and Alliance
intends to discover what took place, Bergan said.
Certain trades executed that day at both the Chicago Stock Exchange and
NYSE were reported to be well below the
stock's prevailing market price at the time of their execution,
including two large blocks - made up of dozens of smaller stop-loss
orders - totaling more than 1.1 million shares traded at the NYSE
(Dow Jones Newswires).
"Are the little people the only ones concerned about
the conduct of those "regulated" (I mean kind of regulated;
they don't even know where to begin the investigation under the current
system! When will SEC ask for help and become a "Team Player"?) by SEC?
"Does anybody really know what time it is? Does anybody really
care (Chicago)?-"little guy"-
-
FDA APPROVES HUMANTROPE
FOR HEIGHT DEFICIENCY
The Food and Drug Administration (FDA) today approved a new
indication for Humatrope (Somatropin, rDNA origin, for injection), a
brand of growth hormone, for the long-term treatment of children with
idiopathic (of unknown origin) short stature, also called non-growth
hormone deficient short stature.
"Short stature" has been defined by the American Association of
Clinical Endocrinologists and the Growth Hormone Research Society as
height more than 2 standard deviations (SD) below the mean for age and
sex. This corresponds to the shortest 2.3 percent of children. This
new indication restricts therapy to children who are even shorter,
specifically more than 2.25 SD below the mean for age and sex, or the
shortest 1.2% of children. For example, for 10-year old boys and
girls, this would correspond to heights of less than 4' 1" inch. This
would further correspond to heights of less than 5' 3" and 4' 11" in
adult men and women, respectively.
Today's approval was based on 2 randomized, multicenter trials,
conducted in approximately 300 children with idiopathic short stature.
The diagnosis of idiopathic short stature was made after excluding
other causes of short stature, including growth hormone deficiency.
The pivotal trial was a randomized, double-blind study in 71
children aged 9-15 years. Patients received injections of either
Humatrope or placebo three times weekly until adult height was
reached. Thirty-three patients contributed final height measurements
after a mean treatment duration of 4.4 years. Mean final height of the
Humatrope patients exceeded that of the placebo patients by
approximately 1.5 inches.
In a second study, patients received one of three increasing doses
of Humatrope, in divided doses six times weekly. The average duration
of treatment to final height was 6.5 years. Final height exceeded that
predicted at the time of enrollment in the majority of patients, and
by up to nearly four inches in some. In the high-dose group, mean
final height exceeded mean height predicted at baseline by nearly
three inches.
The safety profile of Humatrope in children with idiopathic short
stature did not differ from that in children with other conditions for
which growth hormone is indicated.
Various growth hormone products are currently indicated in children
for short stature associated with growth hormone deficiency, chronic
renal insufficiency, Turner syndrome, Prader-Willi syndrome, and in
children born small for gestational age.
Humatrope's new indication for idiopathic short stature is the
first indication for growth hormone in children that specifies a
height restriction (see above).
On June 10, 2003, the application for this new indication was
presented to FDA's Endocrine and Metabolic Advisory Committee for
public discussion and consideration. The advisory committee voted 8-2
in favor of approval.
The manufacturer has advised FDA that it will not engage in
direct-to-consumer advertising of Humatrope and will limit the
marketing of this product for this new use to pediatric
endocrinologists in order to better ensure the proper use of this
product in the indicated pediatric population. In addition, the
manufacturer intends to tightly control the distribution of Humatrope.
Humatrope is manufactured and distributed by Eli Lilly Co. of
Indianapolis, Ind.
Nothing on
this Beat the Press was written by this civilian editor and consumer
advocate.
-
FDA APPROVES ENBREL
TO TREAT ANKYLOSING
SPONDYLITIS
FDA today approved an application for etanercept (trade-name Enbrel),
a genetically engineered protein, for a new indication for treatment of
patients with active ankylosing spondylitis (AS), a chronic inflammatory
disease affecting primarily the lower back and joints. The product is
manufactured by Immunex Corporation, Thousand Oaks, Calif. and marketed
by Amgen and Wyeth Pharmaceuticals. Etanercept is also licensed for
treatment of patients with rheumatoid arthritis, juvenile rheumatoid
arthritis, and psoriatic arthritis.
Approximately 350,000 patients in the United States have AS. The
disease affects men more often than women. Symptoms of the disease may
start in adolescence and are usually present by age 30. Patients often
have lower back pain and stiffness, chest pain, joint pain and swelling,
and tenderness due to the inflammation. In some patients the disease can
cause significant pain and disability for many years.
Currently approved drugs for AS include some non-steroidal
anti-inflammatory drugs (NSAIDS) which are approved to treat the
symptoms of AS. Disease Modifying Anti-Rheumatic Drugs (DMARDS) that are
approved for use in other inflammatory joint diseases are sometimes used
when NSAIDS are ineffective, but none is FDA approved for use in the
treatment of AS.
Etanercept binds to tumor necrosis factor (TNF), a naturally
occurring protein in the body, and inhibits its action. TNF, which
promotes inflammation in the body, is found at elevated levels in the
blood and certain tissues of patients with AS. It is believed that
interference with TNF plays a role in the beneficial effects of
etanercept for AS.
The major efficacy trial of etanercept for AS was a randomized,
double-blind, placebo-controlled study of 277 patients. The study
excluded patients with the most severe forms of AS. After six months of
twice-weekly treatments, 58% of patients who received etanercept showed
significant improvement on a scale that measured pain, function, and
inflammation compared to 23% who received a placebo.
The main side effects of etanercept in the study were similar to
those previously seen for this drug for other indications, including
injection site reactions and upper respiratory infections. The approved
labeling warns physicians about post-marketing reports of serious
infections. The labeling says that Enbrel should not be given to
patients with any active infection, including chronic or localized
infections. It also recommends that patients who develop a new infection
while being treated with Enbrel should be monitored closely.
Amgen will continue to follow patients in the trial to evaluate the
long-term safety of etanercept in patients with AS.
-
UNITED STATES CLEAR ON
ALBERTA, CANADA MAD COW DISEASE DEBACLE
The Food and Drug Administration (FDA) has learned from the
government of Canada that the brain of an eight-year old cow in a remote
area of Alberta has tested positive for bovine spongiform encephalopathy
(BSE, also known as “Mad Cow Disease”).
According to Canadian officials, meat from the cow did not enter the
food supply. The animal had been on the farm in Alberta for three years.
Although BSE has not been shown to be transmitted among cows in a herd,
as a precaution the herd in Alberta is being destroyed.
FDA is working closely with the U.S. Department of Agriculture, other
U.S. agencies, and the appropriate Canadian officials to gather
additional information about this case, including previous owners of the
cow and its location, as well as records concerning animal feed the cow
ate.
To date, no case of BSE has ever been found in the U.S., despite
years of intensive testing for the disease.
After the original outbreak of BSE in the United Kingdom in 1986, the
U.S. government established a comprehensive set of measures designed to
protect Americans and U.S. cattle from BSE. These included a list of
“BSE countries” from which cattle, meat, beef-derived products, and
animal feeds could no longer be exported to the U.S.
As in the past, when individual European countries and Japan
discovered their first cases of BSE, today’s announcement means that
Canada will be added to the list of BSE countries. As a result, cattle,
beef, beef-based products, and animal feed will no longer be allowed to
be exported from Canada to the U.S.
Possible further actions will depend on the findings from the current
investigation of this one confirmed case of BSE in Alberta.
Since 1997, America has been protected from BSE by the prohibition
against using most mammalian protein to manufacture animal feeds given
to “ruminant” animals such as cows, sheep, and goats. The BSE epidemic
in the U.K. is thought to have spread through the addition of such
mammalian protein to the feed consumed by cows. The regulation is
designed to prevent the spread of BSE in the U.S. if a case ever
occurred here.
In 2001, the Harvard Center for Risk Analysis concluded that the
FDA’s “feed rule” provided the nation’s major defense against BSE.
BSE is one of several diseases known as transmissible spongiform
encephalopathies. These diseases are characterized by a long incubation
period, a relatively short clinical course of neurological signs, and
100 percent mortality.
FDA will provide updates on this case of BSE in Alberta as additional
information becomes available.
-
FDA APPROVES "GLEEVEC" FOR
PEDIATRIC LEUKEMIA
The Food and Drug Administration (FDA) today announced the approval
of Gleevec (imatinib mesylate) tablets for the treatment of pediatric
patients with Philadelphia chromosome positive(Ph+)chronic myeloid
leukemia (CML) in chronic phase — a rare, life-threatening form of
cancer that accounts for approximately two percent of all leukemias in
children.
Gleevec is indicated for children whose disease has recurred after
stem cell transplant or who are resistant to interferon alpha therapy.
This drug was approved under the accelerated approval program. The
program helps make products for serious or life-threatening diseases
available earlier in the development process by allowing approval to be
based on a promising effect of the drug, such as tumor shrinkage. As of
yet, there are no controlled trials demonstrating
clinical benefit, such as improvement in disease-related symptoms or
increased survival. Subsequent studies after approval will be conducted
to confirm that the drug has improved survival or other clinical
benefits in pediatric patients.
“Gleevec was originally granted accelerated approval two years ago
for certain kinds of leukemia in adults, and now has been shown to be a
valuable treatment for certain leukemias in children that do not respond
to other treatments,” said FDA Commissioner Mark B. McClellan, M.D.,
Ph.D. “ With follow up studies to confirm its benefits, Gleevec
illustrates the type of significant medical advance for children that
can be achieved quickly under FDA’s accelerated approval program.”
“Today’s approval is the first approval of a new pediatric cancer
drug treatment in over a decade,” added Dr. McClellan. “We hope to see
more products developed that improve pediatric cancer care, and we are
working to facilitate their development and timely approval.”
In addition to its original approved indication for CML refractory to
other treatments in adults, and expansion
to use as a first line treatment for CML, Gleevec was also previously
granted accelerated approval for the treatment of gastrointestinal
stromal cancer in February, 2002.
Today’s accelerated approval of Gleevec for pediatric use is based on
extrapolation of results from Gleevec treated adults with CML together
with good responses in a small number of children.
As a condition of approval Novartis has agreed to conduct pediatric
studies after approval to gain greater insight into the drug’s use in
children.
The most frequently reported adverse events reported with the use of
Gleevec are nausea, vomiting, diarrhea, edema(sometimes severe), and
muscle cramps. A considerable reduction in white blood cells and
platelets was also reported with Gleevec treatment.
The recommended dosage for pediatric populations is 260mg/m2/day. In
children, Gleevec treatment can be given as a once daily dose or,
alternatively, the daily dose may be split in two-once in the morning
and once in the evening.
Gleevec is manufactured by Novartis Pharma AG for Novartis
Pharmaceuticals Corporation located in East Hanover, N.J
-
FDA Announces Smallpox Vaccine
Guidance for Blood Industry
FDA has issued guidance for the blood industry regarding procedures
for properly qualifying potential blood donors who have recently been
inoculated with the smallpox vaccine (vaccinia virus) or those who may
have had other direct exposure to smallpox vaccines.
These recommendations were developed in consultation with experts
on the vaccine virus (smallpox vaccine) at the U.S. Centers for
Disease Control and Prevention and the Department of Defense. They are
preventive measures pertaining to non-emergency smallpox vaccination.
In the event of widespread emergency vaccination due to an actual or
impending smallpox outbreak, the procedures outlined in the guidance
could be modified to adapt to changing risk/benefit assessments and
other public health considerations.
The vaccine virus is closely related to smallpox (variola virus)
and induces an immune response that is protective against smallpox.
The vaccine virus has been used with great success for over 100 years
to protect against smallpox.
FDA is issuing this guidance as a precautionary measure to reduce
the very slight risk of blood borne exposure to the smallpox vaccine
among certain small patient populations that may develop adverse
reactions to the vaccine.
Call on your Senators and Representatives to Stop More Medicare
Payments Cuts...
Congress recessed in late October without taking final
action on pending AMA and APA supported legislation to stop further reductions in Medicare
payments to physicians. The Medicare "update" was cut by 5.4 percent in
2002, and absent action by Congress, an additional cut of roughly 4.4 percent is expected
in 2003, with still more payment update cuts in US civilian neccessary qualifed care.
The cuts are hurting present and future Medicare patients. Why? Because these cuts
are and will continue to drive some doctors out of the business of treating Medicare
patients.
Please add your personal voice to the chorus of people
advising Congress to fix the problem and stop Medicare failure. Call Toll Free
1-866-727-4894 to be connected to the Capitol Hill Switchboard. When you reach the
Capitol Operator, California residents ask for your Senators by name: Barbara Boxer and
Dianne Feistein (out of state citizen mention your all important Senators' name).
When you are connected to their offices, leave the following brief message "in your own words of course":
"As a constituent, I urge you to pass legislation
now, to stop additional cuts in Medicare payments to physicians. These are real cuts
that are hurting my doctors and Medicare patients, like me, who depend on them.
Please stop playing politics with Medicare payments and pass a payment update
"fix" for all of Uncle Sams' neices and nephews now! This action alone
will prove to the world, that Americans care about Americans, and we are still "God's
Country" for the defense of freedom, the health to experience it, and contribute to
the continual improving progress in all areas of human life on "God's Green
Earth". InfoJustice
·
FDA GRANTS CITIZEN'S PETITION SEEKING UNAPPROVED DRUG
CLASSIFICATION FOR "NICOTINE WATER"
Today the Food and Drug Administration (FDA) issued a response to a Citizen's Petition
submitted to the agency regarding the regulation of a product called "Nicotine
Water." Based on several factors, including statements contained in the labeling of
the product, and other evidence of intended use, FDA has determined that this product
should be regarded as an unapproved new drug and cannot be legally marketed as a dietary
supplement.
"FDA's decision underscores our commitment that consumers be protected from drug
products that have not undergone our rigorous review process," said Dr. Lester M.
Crawford, FDA Deputy Commissioner.
The petition was submitted in December of 2001, on behalf of several groups including
the National Center for Tobacco-Free Kids, the American Medical Association, and the
American Lung Association. The petitioners specifically requested that the FDA classify
and regulate "Nicotine Water" as a drug under the Federal Food, Drug, and
Cosmetic Act (the Act), or classify and regulate this product as a food containing an
unapproved food additive under the Act.
FDA has concluded that "Nicotine Water" is an unapproved drug under the Act
because it is intended to treat or mitigate nicotine addiction as a smoking cessation
product. Because nicotine addiction is considered a disease, FDA requires safety and
efficacy data to support any claims intended to treat this disease. After reviewing the
claims on the manufacturer's Internet site, which were submitted with the Citizen's
Petition, FDA concluded "Nicotine Water" is an unapproved drug and may not be
legally sold in the United States until the manufacturer submits a new drug application to
the agency and the agency approves the application.
FDA has also determined "Nicotine Water" which contains as an active
ingredient nicotine or nicotine polacrilex, cannot be legally marketed as a dietary
supplement. Although "Nicotine Water" is promoted by the manufacturer as a
dietary supplement, this product does not meet the statutory definition of a dietary
supplement. Under the Act, a "dietary supplement" does not include a product
that contains an active ingredient that FDA has already approved for use in a drug.
Because the nicotine and nicotine polacrilex in "Nicotine Water" are both active
ingredients in FDA-approved drugs (such as Nicoderm CQ, Prostep, Habitrol, and Nicorette)
"Nicotine Water" cannot be marketed as a dietary supplement.
In light of these determinations, FDA will notify manufacturers of "Nicotine
Water" that this product cannot be marketed without new drug approval by the agency.
FDA will continue to monitor the marketplace to ensure that consumers are protected from
unapproved drug products.
FTC Charges Three Top-selling
Electronic Abdominal Exercise Belts with Making False Claims
Alleges Electronic Abdominal
Gadgets Won't Provide Six-Pack Abs
"Now you can get rock hard abs with no
sweat"
"Lose 4 Inches in 30 Days Guaranteed"
"30% More Effective Than Normal Exercise"
"10 Minutes = 600 Sit-Ups"
These are the types of claims the Federal Trade Commission has challenged in complaints
filed in federal district courts against three widely advertised electronic abdominal
exercise belts - AB Energizer, AbTronic, and Fast Abs. The FTC alleges that the marketers
of the devices, which use electronic muscle stimulation (EMS), have falsely advertised
that users will get "six pack" or "washboard" abs without exercise.
"For years, marketers of diet and exercise products have been preying on
overweight, out-of-shape consumers by hawking false hope in a pill, false hope in a
bottle, and, now, in a belt," said FTC Chairman Timothy J. Muris.
"Unfortunately, there are no magic pills, potions, or pulsators for losing weight and
getting into shape. The only winning combination is changing your diet and exercise."
The FTC filed three separate complaints against the following defendants:
- AB Energizer marketers: Electronic Products Distribution, L.L.C., based
in San Diego, California, and its general partners, Thomas Nelson and Holly Hernandez,
also known as Holly Bryan; Energizer Products, Inc., based in Tarzana, California; Ab
Energizer, L.L.C., based in San Diego, California; and AbFlex USA, Inc., also located in
San Diego, and its president, Martin Van Der Hoeven;
- AbTronic marketers: Hudson Berkley Corporation, based in Las Vegas,
Nevada, and also doing business as Hudson Berkeley, Inc., and its officer and director,
Matthias Granic; Bismarck Labs Corporation, based in Palm Springs, California and also
doing business as BLC Bismarck Labs Corporation; TMI Tricom Marketing, Inc., a Delaware
corporation; CCI CAD CAM Industries Ltd., Inc., located in Hong Kong; and Bernd Ebert, a
director and officer of BLC, managing director of TMI, and president of CCI; and
- Fast Abs marketers: United Fitness of America, L.L.C., based in
Ventura, California, and its sole manager, George Sylva; and Tristar Products, Inc., based
in Parsippany, New Jersey, and its president, Kishore Mirchandani, also known as Keith
Mirchandani.
According to the FTC, the defendants sold their devices through heavily aired,
30-minute infomercials on national cable television stations such as USA, TNN, Lifetime,
E!, FX, and Comedy Central. Each of the infomercials has been among the ten most
frequently aired infomercials in weekly U.S. rankings and has aired well over a thousand
times. The infomercials feature fitness professionals who tout the products' efficacy,
user testimonials, photos of models sporting trim, sculpted midsections, and purported
expert opinions from health care professionals. The AB Energizer and AbTronic marketers
also aired shorter television commercials. In addition, Fast Abs has been advertised in
national newspaper magazines such as Parade, and mailed circulars such as
Clipper
Magazine.
The defendants advertised the three devices through Internet Web sites and at national
retail outlets. In addition, the defendants made claims on the packaging for the three
products, which the FTC also allege were false and deceptive. The products sell for about
$40-$120.
The FTC's complaints allege that the advertisements for the three ab devices falsely
represent that:
- the ab devices cause fat loss and inch loss;
- the ab devices will give users well-defined abdominal muscles (e.g., "rock
hard," "six pack" or "washboard" abs); and
- use of the ab devices is equivalent to (and, for AbTronic and Fast Abs, superior to)
conventional abdominal exercises, such as sit-ups or crunches.
The complaint against the AB Energizer defendants also alleges that they falsely
represented that the device will cause weight loss. The AbTronic complaint alleges that
the defendants falsely represented that the device eliminates cellulite, and that a
scientific study proves that use of the AbTronic improves abdominal strength better than
exercise alone.
The FTC complaints further allege that the advertising for all three devices falsely
claimed that the devices are safe for all users and failed to disclose, or failed to
disclose adequately, warnings about health hazards for some people. According to the FDA
and leading texts on EMS therapy, EMS devices should not be used by persons with certain
conditions, including implanted pacemakers or other implanted metallic or electronic
devices, swollen or inflamed areas (such as phlebitis), or cancerous lesions.
Additionally, safety of EMS during pregnancy has not been established. The AbTronic and
Fast Abs complaints also allege that the marketers falsely advertised that the products
are safe for use over the chest area.
In addition to the false advertising allegations, the FTC complaints challenge refund,
shipping, and warranty practices. The FTC alleges that all of the defendants
misrepresented their "money-back guarantees" and, in many cases, failed to
provide timely refunds. The FTC also alleges that marketers for all three devices violated
the FTC's Mail or Telephone Order Merchandise Rule by failing to ship their direct-order
products within the promised shipment time (and in some cases, failing to ship the
products at all), and failing either to notify consumers of the delay or cancel the order
and make a prompt and full refund. Further, the FTC alleges that the Fast Abs infomercial
represented that the product comes with a one-year limited warranty, when in fact, some
consumers received only a 30-day limited warranty with the product.
The FTC is seeking permanent injunctions in each of these cases to prohibit the
defendants from making false or deceptive advertising claims, stop them from engaging in
other deceptive marketing practices, and require them to pay redress to consumers.
The U.S. Food and Drug Administration and the Napa County, California District
Attorney's Office provided assistance on these cases.
The Commission vote to authorize staff to file the three complaints in the appropriate
federal district courts was 5-0. The Ab Energizer matter was filed in the U.S. District
Court for the Southern District of California, in San Diego, on May 7, 2002. The Fast Abs
and AbTronics matters were filed in the U.S. District Court, District of Nevada, in Las
Vegas, on May 7, 2002.
Consumer Tips
The FTC has updated two consumer publications about exercise equipment: "Avoiding
the Muscle Hustle" www.ftc.gov/bcp/conline/pubs/alerts/musclealrt.htm
and "Pump Fiction: When Marketers Overextend Their Fitness Claims." www.ftc.gov/bcp/conline/pubs/products/pumpfict.htm
These materials offer tips to consider and questions to ask before buying exercise
equipment, including:
- Ignore claims that an exercise machine or device can provide long-lasting, easy,
"no-sweat" results in a short time. These claims are false: You can't get the
benefits of exercise unless you exercise.
- Don't fall for claims that a product can burn fat off a particular part of the body -
for example, the stomach, hips or buttocks. Achieving a major change in your appearance
requires sensible eating and regular exercise that works the whole body.
- Read the ad's fine print. The advertised results may be based on more than just using a
machine; it also may be based on restricting calories.
- Be skeptical of testimonials and before-and-after pictures from "satisfied"
customers. Their experiences may not be typical. Just because one person had success with
the equipment doesn't mean you will, too.
- Get details on warranties, guarantees and return policies. A "30-day money-back
guarantee" may not sound as good if you have to pay shipping on the equipment you
want to "return to sender."
- Check out the company's customer and support services. Call the advertised toll-free
numbers to get an idea of how easy it is to reach a company representative and how helpful
he or she is.
FDA-FCC Cellular Phone and Radio
Frequency
Energy Website Posted for Public Use and Comment
The Food and Drug Administration (FDA) and the Federal Communications Commission (FCC)
have established a joint web site, Cell Phone
Facts, to provide consumer information regarding cellular phones and
radiofrequency (RF) energy. This web site provides the public with information from both
government agencies involved in the regulation of cell phones (also known as wireless,
mobile, or PCS phones) and their base stations. It provides a review of how cell phones
work and answers questions raised about their safety. It also includes a link to the FCC's
web site that contains additional information about radiofrequency safety as it relates to
other sources of RF energy.
Most of the concerns about cell phone safety involve the phone's production of RF
energy from a source close to the head or body of the user. The web site explains that
although cell phones use RF to transmit calls, the FCC limits the amount of RF energy that
may be produced by a cell phone to safe levels and the levels permitted are far below the
levels determined by scientific experts to have the potential for an adverse effect on
humans. It also observes that while no scientific evidence has been published
demonstrating harm from short- term exposures to low levels of RF energy, studies are now
underway to look at the possible risks of long-term exposures. The results of any such
studies will also be posted on the web site and both agencies will take follow-up action
as appropriate.
The new web site summarizes the government's safety standards for cell phones and
describes the role of each agency in RF safety regulation. It also explains what RF energy
is, how it is used, and how it is measured; how the current safety standards were
established; the role of local and state governments; and where to obtain additional
information on related topics from other sources. The FDA and the FCC will periodically
update the website in response to queries and comments received from the public and as new
information becomes available.
The FDA-FCC RF safety web site is available for public use and comment at www.fda.gov/cellphones and www.fcc.gov/cellphones
FDA CLEARS NEW RADIATION DEVICE TREATMENT FOR
BREAST CANCER
FDA today cleared a new medical device that provides another option for radiation
treatment for women who have had a cancerous lump removed from their breast (lumpectomy).
The device, a brachytherapy applicator, is designed to irradiate the surgical site from
which the lump has been removed, with minimal irradiation of the surrounding tissue.
(Brachytherapy is radiation treatment in which the source of radiation is close to the
area being treated.)
The new device is the MammoSite Radiation Therapy System, made by Proxima Therapeutics,
Inc., of Alpharetta, Ga. It consists of a hollow catheter to which an inflatable balloon
it attached.
The device is implanted into the breast at the site of the lumpectomy, and the balloon
is inflated. A radioactive source is then placed into the catheter. The balloon acts to
center the radiation source within the wound. After a series of treatments are
completed--typically over several days--the catheter is removed.
The device is intended to be used primarily to treat breast cancer in its early stages
when there is no need to remove the whole breast. It does not replace whole breast
irradiation in women who need that treatment.
FDA cleared the device based on information that showed it was comparable in safety and
effectiveness to other devices used to deliver brachytherapy to the breast and other body
parts. Such information included clinical data from 25 women at eight medical centers who
had the device implanted after lumpectomy. The study showed that this new method of
delivering brachytherapy was relatively simple and did not create increased risk to the
patient.
As a condition for clearance, FDA is requiring Proxima Therapeutics to include a
warning in the product labeling that the safety and effectiveness of MammoSite as a
replacement for whole breast irradiation to treat breast cancer has not been established.
Dietary Supplement Firm Signs Consent Decree with
FDA to Stop Selling Product Containing Ephedrine Hydrochloride
The Food and Drug Administration today announced that Biogenics Inc., of St. George,
Utah, doing business as E'OLA International, has signed a consent decree that prohibits
the firm from manufacturing and distributing violative products. These include AMP II Pro
Drops, any product containing ephedrine hydrochloride, or any synthetic ephedrine
alkaloid, or any drug product that is a new drug not approved by FDA.
"This action is yet another example of FDA's strong commitment to protecting the
public from the dangers of unlawfully marketed drug products," said Lester M.
Crawford, D.V.M., Ph.D., Deputy Commissioner of The Food and Drug Administration.
The decree also gives FDA the authority to order the firm to discontinue the marketing
of and recall any
products that violate the law in the future. The decree was signed Friday, April 12, 2002,
by United States District Court Judge Tena Campbell in Salt Lake City, Utah.
On October 30, 2001, at the request of the FDA, US Marshals seized $2.8 million worth
of E'OLA's product, known as AMP II Pro Drops. Previous FDA inspections found that the
products contain a drug, ephedrine hydrochloride, but are labeled as a dietary supplement
for use in weight loss. These E'OLA products violate the law because drug ingredients are
prohibited for use in dietary supplements.
Ephedrine hydrochloride has been approved as a drug by FDA since 1948, and therefore
cannot be legally marketed as a dietary supplement. E'OLA also marketed its product as a
treatment for obesity. Products marketed to treat diseases are drugs.
The product is also misbranded because its labeling fails to bear adequate directions
for its intended use.
As a result of this consent decree, E'OLA International will destroy the seized articles
at its own expense under the supervision of a Department of Health and Human Services
representative within 25 days
CALIFORNIA SENATOR WARNS THAT
COMPANIES MANIPULATED THE ENERGY CRISIS
A California state lawmaker investigating the state's recent energy woes joined an
industry coalition Wednesday to warn of broad U.S. vulnerability to energy-market
manipulation.
At a press briefing, California State Senator Joseph Dunn, R-Garden Grove, said he has new
evidence Enron Corp. (ENRNQ) and other energy suppliers fixed prices during the state's
2000-2001 energy crisis.
"Enron and its clones promised greater efficiency and cheaper energy prices, but have
delivered just the opposite," Dunn said, citing an estimated $9 billion in costs to
the state from the crisis.
Dunn has been leading a 14-month study of the crisis, subpoenaing millions of documents
from market participants and financial institutions. He says the evidence shows that
unregulated marketing companies with control of 64% of interstate gas pipeline capacity
into California used their power to drive the state's natural gas prices to unprecedented
peaks in December 2000.
Unregulated companies also controlled 74% of California's gas-fired electricity generation
during the 2000-2001 winter, he said. Since companies controlled both natural gas and
power generation, they were able to bypass emergency wholesale power price caps imposed by
the federal government, he said.
Dunn said the increasing use of gas-fired power generation makes other parts of the
country similarly vulnerable. "This is not a California problem. It surfaced here
first, but stay tuned," he said.
The state senator was speaking in a teleconference with representatives of a group of gas
producers and energy utilities calling itself the Coalition for Energy Market Integrity
and Transparency.
Apache Corp. (APA) Chief Executive Raymond Plank, a member of the coalition, said the
California and Enron debacles demonstrate the conflicts of interest that "middle
men" have under current U.S. energy regulations. "Don't think that there's only
one company (like Enron)," Plank said. Apache is a Houston-based natural gas and oil
producer.
"The marketer-speculators are destroying North America's natural gas business by
promoting unwarranted price volatility," Plank said. "Producers have no idea
where the price of gas is going to be tomorrow, much less a year or two from now...so we
drill fewer and fewer wells."
Plank blamed energy marketers like Dynegy Inc. (DYN), El Paso Corp. (EP) and Williams Cos.
(WMB) for killing a legislative proposal before the Senate that would have allowed federal
oversight of over-the-counter energy markets, including online systems. "The last
thing they want is the bright light of day shining on their operations," he said.
Other members of the coalition include the American Public Gas Association, the American
Public Power Association, the Texas Independent Producers and Royalty Owners Association,
and numerous local utility companies.
TRAUMATIC BRAIN INJURY- PRECIOUS CUTTING EDGE
INFODATA FROM CDC
Although injuries are the second leading cause of death among American Indians and
Alaska Natives (AI/ANs), little is known about non-fatal injuries in this population. This
study describes the causes and impact of one type of injury— traumatic brain injury
(TBI) on AI/ANs using Indian Health Service (IHS), tribal or contract hospital discharge
data.
Between 1992-1996, IHS, tribal, or contract care hospitals recorded 4,491 TBI-related
hospitalizations among AI/ANs with an average length of stay of 4.7 days. Males had almost
three times as many TBIs as females.
The major causes of hospitalizations for TBI were motor vehicle collisions (24%),
assaults (17%), and falls (16%). These findings indicate that falls contribute to TBI
among AI/AN almost as much as assaults.
Among AI/ANs age 15-24, motor vehicle collisions were the most common cause of TBI. For
young adults 25-34 years and 35-44 years, assaults were the most likely cause of TBI,
although only 5% of cases involved firearms. For youth 0-14 years and adults 45 years and
older, falls were the leading cause of injury.
The highest number of hospitalized TBIs among AI/ANs were found in the Northern Plain
states and Alaska.
In a previous CDC study, the Navajo Nation has shown that enactment and enforcement of
a mandatory seat belt law led to increases in seat belt use and a 29% reduction in
motor-vehicle-related injuries among Navajo Nation residents.
FDA WARNS ABOUT POSSIBLE ENTEROBACTER
SAKAZAKII INFECTIONS IN HOSPITALIZED NEWBORNS FED POWDERED INFANT FORMULAS
Warning Does Not Apply to Liquid Forms of Infant Formula
FDA today alerted health care professionals about the risk of Enterobacter sakazakii
(E.sakazakii) infections in hospitalized newborn infants, particularly premature
infants or other immuno-compromised infants fed powdered infant formulas. This alert
issued by FDA is targeted to concerns for immuno-compromised infants in hospital settings.
The FDA is not aware of E. sakazakii infections among healthy full term infants in
home settings. In addition, this alert does not involve the use of liquid infant formulas.
E. sakazakii is an emerging foodborne pathogen that can cause sepsis,
meningitis, or necrotizing enterocolitis in newborn infants, particularly premature
infants or other infants with weakened immune systems. Over the last several years,
investigations of several outbreaks of E. sakazakii infection occurring in neonatal
intensive care units worldwide have shown the outbreak to be associated with milk-based
powdered infant formulas.
Recently, the U. S. Centers for Disease Control and Prevention (CDC) investigated a
fatal E. sakazakii meningitis case in a neonatal intensive care unit in the United
States. According to the CDC, the use of milk-based powdered formula was a likely factor
in the infection of this child. The details of CDC's investigation will be outlined in an
upcoming edition of the Morbidity and Mortality Weekly Report (MMWR).
The FDA letter to health professionals, which is available at http://www.cfsan.fda.gov/~dms/inf-ltr3.html,
provides recommendations for minimizing the risk in those circumstances when a powdered
formula must be used for premature or immuno-compromised infants.
FDA urges health care providers to report adverse events associated with the use of
infant formulas as soon as possible to FDA's MedWatch program by calling their toll-free
number (1-800-332-1088) or through the Internet (http://www.fda.gov/medwatch). Healthcare
providers should report invasive disease in infants due to
E. sakazakii, particularly bloodstream infection or meningitis with onset in the
healthcare setting, to CDC's Division of Healthcare Quality Promotion (1-800-893-0485).
SMOKING COSTS NATION $159 BILLION EACH YEAR IN
HEALTH COSTS AND LOST PRODUCTIVITY.
Each pack of cigarettes sold in the United States costs the nation an estimated $7.18
in medical care costs and lost productivity, the Centers for Disease Control and
Prevention (CDC) reported today.
In a study of deaths related to smoking, years of life lost, and economic costs, CDC
found that smoking continues to be the leading cause of preventable death in the United
States, resulting in an estimated 440,000 premature deaths annually from 1995 through
1999. On average, adult men and women smokers lost 13.2 and 14.5 years of life,
respectively, because they smoked.
Economic costs during the same period were $81.9 billion in productivity losses from
deaths (average for 1995-1999) and $75.5 billion in excess medical expenditures in 1998,
for a total of more than $150 billion, according to the report. The reported medical and
productivity losses were larger than previous estimates of $53 billion and $43 billion,
respectively.
"The fact that nearly half a million Americans lose their lives each year because
of smoking-related illnesses is a significant public health tragedy," said Dr. David
Fleming, acting director, CDC. "It's important now more than ever that states and
local communities put in place comprehensive tobacco control programs to stem this tidal
wave of preventable deaths."
According to the analysis, for each of the 22 billion packs of cigarettes sold in the
United States in 1999, $3.45 was spent on medical care related to smoking, compared with
the previous 1993 estimate of $2.06 per pack. Another $3.73 per pack was spent on
productivity losses from smoking. Overall, the economic cost of smoking equaled about
$3,391 per smoker per year.
"The stunning toll that smoking takes on life is unacceptable," said
Rosemarie Henson, director of CDC's Office on Smoking and Health. "States and
communities can and should do more to reduce the impact of smoking on the physical and
financial health of their communities."
Despite recent declines, young people in the United States are still using tobacco at a
high rate: 34.5 percent of high school students and 15.1 percent of middle school students
currently use some form of tobacco (cigarettes, smokeless, cigars, pipes, bidis, or
kreteks). Every day, more than 2,200 young people under the age of 18 become daily
smokers.
Other findings from the new study include these:
- Each year from 1995 through 1999, smoking caused more than 264,000 deaths in men and
more than 178,000 deaths in women.
- Among adults, most deaths were from lung cancer (124,813), heart disease (81,976) and
lung disease (64,735).
- Smoking-related cancer and lung disease deaths in women increased from 1995 to 1999.
- Smoking during pregnancy resulted in more than 1,000 infant deaths annually.
- Neonatal costs were $366 million--$704 per pregnant smoker—in 1996.
The CDC is also releasing Tobacco Control State Highlights 2002: The Impact and
Opportunity. This report, which provides current data on tobacco funding for states
and the District of Columbia, can be viewed or downloaded today at http://www.cdc.gov/tobacco/. More information on
CDC's tobacco control activities can be found at CDC's Tobacco Information and Prevention
Source (TIPS) Web site at http://www.cdc.gov/tobacco/.
In addition to these reports, the CDC is unveiling the Internet-based Smoking
Attributable Mortality, Morbidity, and Economic Costs (SAMMEC) software. SAMMEC is a first
of its kind online application that allows users to estimated the health and
health-related economic consequences of smoking to adults and infants. Users can register
for and use the software at http://www.cdc.gov/tobacco/sammec.htm.
FDA WARNS SELLERS OF NICOTINE LOLLIPOPS & LIP
BALM THAT THEIR PRODUCTS ARE ILLEGAL
Today FDA issued warning letters to three pharmacies that are selling "nicotine
lollipops" and/or nicotine "lip balm" over the Internet. The letters inform
the pharmacies that FDA has found their nicotine lollipops and lip balm to be illegal.
Based on statements from the pharmacies' Internet sites, the products are promoted as aids
for smoking cessation or to treat nicotine addiction.
FDA is concerned about the health risk of these products because the appear to be
compounded and dispensed without a doctor's prescription, contain a form of nicotine that
is not used in FDA-approved smoking cessation products, and because these candy-like
products present a risk of accidental use by children.
The products cited in the letters include compounds incorporating nicotine salicylate,
natural sweeteners, and flavorings in a sugar-free base and are available in ˝ mg., 1
mg., 2 mg., and 4 mg. dosages. The claims on the websites include that the products help
alleviate the "hand to mouth fixation" associated with smoking and are a
"convenient, tasty way" to replace the cigarette habit. After investigating and
carefully assessing these websites, FDA has determined that the pharmacies' nicotine
lollipops and nicotine lip balm are intended for use as "drugs" and appear to be
illegal for the following reasons:
- They are compounded and dispensed without a doctor's prescription.
- They are unapproved new drugs which need, but do not have, FDA approval.
- They are made from a drug substance, nicotine salicylate, which is not permitted for use
by pharmacists in compounding drugs. The FDA-approved smoking cessation products are made
from different forms of nicotine.
- They are misbranded because their labeling does not have adequate directions for the
uses for which they are being offered and does not have adequate warnings against use by
children.
FDA is requesting a response from the pharmacies in writing within 15 days of receipt
of the warning letters stating the action the firms will take to discontinue marketing of
these drug products. Failure to do so may result in further regulatory action, potentially
including a seizure or injunction action. FDA will take appropriate action to protect the
public health.
Dell Computer should be Del (delete) in
purchasing books.
As most of you know, for one year now, this
examiner, has been morally dedicated to fulfill this presidents national agenda;
(2002 FDA SCIENCE FORUM: BUILDING A
MULTIDISCIPLINARY FOUNDATION)
of bringing
multidisciplinary care to our neighborhoods, in the effort of fulfilling America's health
care destiny. Thus I have had to reduce my consumer protection writings until
someone in the Acadmy steps forward or I have additional "time".
AGAIN, after viewing a Dell Computer Add for a
Pentium IV 1.8 with a 17" monitor for thirteen hundred and change I investigated the
necessity of purchasing new computers for the corporation either as an upgrade or
addition. I still have the magazine albeit still current issue, which clearly
depicts a lovely large 17" viewable monitor. I found that with Compaq for just
a little more money, I could essentially get the same computer with far greater
innovation. One of the innovations I liked was that you could impute analog or
digital signals directly into the computer, and use its soft wear to make my own CD's.
For example, I could plug directly into my computer from my TV, VCR, CAMC, etc.
absent the need for any external devices. I called Dell to inquire the cost of the
Dell System above with special card inside. Of course they claimed that's why they
are the best company taking everyone's business and on and on! I went over all
details, and they were paid up front Two thousand three hundred eighty eighty dollars and
change. Far more that the original thirteen hundred system they still advertise.
Of course to make the board I wanted work correctly I would need double the ram and
double the hard drive size. I believed them.
About twelve days later my nightnear arrived at
my main office of three. In fact they knew if the system worked out well for this
office, I was to purchase another within a few weeks. Well, I opened the new third
office yesterday!
In any event right off the bat I knew something
was wrong because there were four boxes and there should only have been three. I
made the joke, "Gee, I hope they didn't forget to put my board in"! Since
Dell alleges they built this just for me and it went through extensive testing as all dell
computers do. Ha Ha. Everything should have gone normally! Stay tuned
for this one takes the Poor Service, Poor Construction, Poor
Consumer Business Award. InfoJustice
Tips for the Savvy Supplement User: Making
Informed Decisions
The choice to use a dietary supplement can be a wise decision that provides health
benefits. However, under certain circumstances, these products may be unnecessary for
good health or they may even create unexpected risks. The Food and Drug Administration,
health professionals, and other health-related organizations receive many inquiries each
year from consumers seeking health-related information, especially about dietary
supplements. Clearly, people choosing to supplement their diets with herbals, vitamins,
minerals, or other substances want to know more about the products they choose so that
they can make informed decisions about them.
Given the abundance and conflicting nature of information now available about dietary
supplements, you may need help to sort the reliable information from the questionable. The
FDA's Center for Food Safety and Applied Nutrition has prepared these tips and resources
to help you become a savvy dietary supplement user. The principles underlying these tips
are similar to those principles a savvy consumer would use for any product.
Basic Points to Consider
- Do I need to think about my total diet?
Yes. Dietary supplements are intended to supplement the diets of some people, but not to
replace the balance of the variety of foods important to a healthy diet. While you need
enough nutrients, too much of some nutrients can cause problems. You can find information
on the functions and potential benefits of vitamins and minerals, as well as upper safe
limits for nutrients, on the National Academy of Sciences Web site at ww.iom.edu/iom/iomhome.nsf/Pages/FNB+Reports.
- Should I check with my doctor or health-care provider before using a supplement?
This is a good idea, especially for certain population groups. Dietary supplements may not
be risk-free under certain circumstances. If you are pregnant, nursing a baby, or have a
chronic medical condition, such as diabetes, hypertension or heart disease, be sure to
consult your doctor or pharmacist before purchasing or taking any supplement. While
vitamin and mineral supplements are widely used and generally considered safe for
children, you may wish to check with your doctor or pharmacist before giving these or any
other dietary supplements to your child. If you plan to use a dietary supplement in place
of drugs or in combination with any drug, tell your health-care provider first. Many
supplements contain active ingredients that have strong biological effects and their
safety is not always assured in all users. If you have certain health conditions and take
these products, you may be placing yourself at risk.
- Some supplements may interact with prescription and over-the-counter (OTC) medicines.
Taking a combination of supplements or using these products together with medications
(whether prescription or OTC drugs) could, under certain circumstances, produce adverse
effects, some of which could be life-threatening. Be alert to advisories about these
products, whether taken alone or in combination. For example: Coumadin (a prescription
medicine), ginkgo biloba (an herbal supplement), aspirin (an OTC drug) and vitamin E (a
vitamin supplement) can each thin the blood, and taking any of these products together can
increase the potential for internal bleeding. Combining St. John's wort with certain HIV
drugs significantly reduces their effectiveness. St. John's wort may also reduce the
effectiveness of prescription drugs for heart disease, depression, seizures, certain
cancers, or oral contraceptives.
- Some supplements can have unwanted effects during surgery.
It is important to fully inform your doctor about the vitamins, minerals, herbals or any
other supplements you are taking, especially before elective surgery. You may be asked to
stop taking these products at least two to three weeks ahead of the procedure to avoid
potentially dangerous supplement/drug interactions--such as changes in heart rate, blood
pressure and increased bleeding--that could adversely affect the outcome of your surgery.
- Adverse effects from the use of dietary supplements should be reported to the FDA.
You, your health-care provider, or anyone may report a serious adverse event or illness
directly to the FDA if you believe it is related to the use of any dietary supplement
product. Report these concerns to MedWatch, the FDA's safety information and adverse event
reporting system, by calling 1-800-FDA-1088, by fax at 1-800-FDA-0178 or online at www.fda.gov/medwatch/how.htm. The FDA would
like to know whenever you think a product caused you a serious problem, even if you are
not sure that the product was the cause, and even if you do not visit a doctor or clinic.
In addition to communicating with the FDA online or by phone, you may use the MedWatch
form available from the FDA Web site.
- Who is responsible for ensuring the safety and efficacy of dietary supplements?
Under the law, manufacturers of dietary supplements are responsible for making sure their
products are safe before they go to market. They are also responsible for determining that
the claims on their labels are accurate and truthful. Dietary supplement products are not
reviewed by the government before they are marketed, but the FDA has the responsibility to
take action against any unsafe dietary supplement product that reaches the market. If the
FDA can prove that claims on marketed dietary supplement products are false and
misleading, the agency may take action against products with such claims.
Tips on Searching the Web
When searching on the Web, try using directory sites of respected organizations, rather
than doing blind searches with a search engine. Ask yourself the following questions:
- Who operates the site?
Is the site run by the government, a university, or a reputable medical or health-related
association (such as the American Medical Association, American Diabetes Association,
American Heart Association, National Institutes of Health, National Academy of Sciences,
or the FDA)? Is the information written or reviewed by qualified health professionals,
experts in the field, academia, government or the medical community?
- What is the purpose of the site?
Is the purpose of the site to objectively educate the public or just to sell a product? Be
aware of practitioners or organizations whose main interest is in marketing products,
either directly or through sites with which they are linked. Commercial sites should
clearly distinguish scientific information from advertisements. Most nonprofit and
government sites contain no advertising, and access to the site and materials offered are
usually free.
- What is the source of the information and does it have any references?
Has the study been reviewed by recognized scientific experts and published in reputable
peer-reviewed scientific journals, such as The New England Journal of Medicine?
Does the information say "some studies show…" or does it state where the
study is listed so that you can check the authenticity of the references? For example, can
the study be found in the National Library of Medicine's database of literature citations
(www.ncbi.nlm.nih.gov/PubMed/)?
- Is the information current?
Check the date when the material was posted or updated. Often new research or other
findings are not reflected in old material; for example, side effects or interactions with
other products or new evidence that might have changed earlier thinking. Ideally, health
and medical sites should be updated frequently.
- How reliable are the Internet and e-mail solicitations? While the Internet is a rich
source of health information, it is also an easy vehicle for spreading myths, hoaxes and
rumors about alleged news, studies, products or findings. To avoid falling prey to such
hoaxes, be skeptical and watch out for overly emphatic language with UPPERCASE LETTERS and
lots of exclamation points!!!! Beware of such phrases such as: "This is not a
hoax" or "Send this to everyone you know."
More Tips and To-Do's
- Ask yourself: Does it sound too good to be true?
Do the claims for the product seem exaggerated or unrealistic? Are there simplistic
conclusions being drawn from a complex study to sell a product? While the Web can be a
valuable source of accurate, reliable information, it also has a wealth of misinformation
that may not be obvious. Learn to distinguish hype from evidence-based science.
Nonsensical lingo can sound very convincing. Also, be skeptical about anecdotal
information from persons who have no formal training in nutrition or botanicals, or
personal testimonials (from store employees, friends, or online chat rooms and message
boards) about incredible benefits or results obtained from using a product. Question these
people on their training and knowledge in nutrition or medicine.
- Think twice about chasing the latest headline.
Sound health advice is generally based on a body of research, not a single study. Be wary
of results claiming a "quick fix" that depart from previous research and
scientific beliefs. Keep in mind science does not proceed by dramatic breakthroughs, but
by taking many small steps, slowly building towards a consensus. Furthermore, news stories
about the latest scientific study, especially those on TV or radio, are often too brief to
include important details that may apply to you or allow you to make an informed decision.
- Check your assumptions about the following:
Questionable Assumption #1 -- "Even if a product may not help me, it at least
won't hurt me."
It's best not to assume that this will always be true. When consumed in high enough
amounts, for a long enough time, or in combination with certain other substances, all
chemicals can be toxic, including nutrients, plant components, and other biologically
active ingredients.
Questionable Assumption #2 -- "When I see the term 'natural,' it means that a
product is healthful and safe."
Consumers can be misled if they assume this term assures wholesomeness, or that these
food-like substances necessarily have milder effects, which makes them safer to use than
drugs. The term "natural" on labels is not well-defined and is sometimes used
ambiguously to imply unsubstantiated benefits or safety. For example, many weight-loss
products claim to be "natural" or "herbal" but this doesn't
necessarily make them safe. Their ingredients may interact with drugs or may be dangerous
for people with certain medical conditions.
Questionable Assumption #3 -- "A product is safe when there is no cautionary
information on the product label."
Dietary supplement manufacturers may not necessarily include warnings about potential
adverse effects on the labels of their products. If consumers want to know about the
safety of a specific dietary supplement, they should contact the manufacturer of that
brand directly. It is the manufacturer's responsibility to determine that the supplement
it produces or distributes is safe and that there is substantiated evidence that the label
claims are truthful and not misleading.
Questionable Assumption #4 -- "A recall of a harmful product guarantees
that all such harmful products will be immediately and completely removed from the
marketplace."
A product recall of a dietary supplement is voluntary and, while many manufacturers do
their best, a recall does not necessarily remove all harmful products from the
marketplace.
- Contact the manufacturer for more information about the specific product that you are
purchasing.
If you cannot tell whether the product you are purchasing meets the same standards as
those used in the research studies you read about, check with the manufacturer or
distributor. Ask to speak to someone who can address your questions, some of which may
include:
- What information does the firm have to substantiate the claims made for the product? Be
aware that sometimes firms supply so-called "proof" of their claims by citing
undocumented reports from satisfied consumers, or "internal" graphs and charts
that could be mistaken for evidence-based research.
- Does the firm have information to share about tests it has conducted on the safety or
efficacy of the ingredients in the product?
- Does the firm have a quality control system in place to determine if the product
actually contains what is stated on the label and is free of contaminants?
- Has the firm received any adverse event reports from consumers using their products?
Overweight, Obesity Threaten U.S. Health Gains
Health problems resulting from overweight and obesity could reverse many of the health
gains achieved in the United States in recent decades, according to former Surgeon General
David Satcher.
A report issued in December titled The Surgeon General's Call to Action to Prevent
and Decrease Overweight and Obesity outlines strategies that communities can use in
helping to address the problems. Options include requiring physical education at all
school grades, providing more healthy food options on school campuses, and providing safe
and accessible recreational facilities for residents of all ages.
"Overweight and obesity may soon cause as much preventable disease and death as
cigarette smoking," says Satcher, whose term expired Feb. 13. "People tend to
think of overweight and obesity as strictly a personal matter, but there is much that
communities can and should do to address these problems."
About 300,000 U.S. deaths a year are associated with obesity and overweight (compared
to more than 400,000 deaths a year associated with cigarette smoking). The total direct
and indirect costs attributed to overweight and obesity amounted to $117 billion in 2000.
In 1999, an estimated 61 percent of U.S. adults were overweight, along with 13 percent
of children and adolescents. Obesity among adults has doubled since 1980, while overweight
among adolescents has tripled. Only 3 percent of all Americans meet at least four of the
five federal Food Guide Pyramid recommendations for the intake of grains, fruits,
vegetables, dairy products, and meats. And less than one-third of Americans meet the
federal recommendations to engage in at least 30 minutes of moderate physical activity at
least five days a week, while 40 percent of adults engage in no leisure-time physical
activity at all.
"Overweight and obesity are among the most pressing new health challenges we face
today," says Tommy G. Thompson, secretary of Health and Human Services. "Our
modern environment has allowed these conditions to increase at alarming rates and become a
growing health problem for our nation. By confronting these conditions, we have tremendous
opportunities to prevent the unnecessary disease and disability they portend for our
future."
While the prevalence of overweight and obesity has increased for both genders and
across all races and ethnic and age groups, disparities do exist. In women, overweight and
obesity are higher among members of racial and ethnic minority populations than in
non-Hispanic white women. And, Mexican-American men have a higher prevalence of overweight
and obesity than non-Hispanic men, while non-Hispanic white men have a greater prevalence
than non-Hispanic black men. Members of lower-income families generally experience a
greater prevalence than those from higher-income families.
Already, these trends are associated with dramatic increases in conditions such as
asthma, and in type 2 diabetes among children. Satcher says failure to address overweight
and obesity "could wipe out some of the gains we've made in areas such as heart
disease, several forms of cancer, and other chronic health problems."
In preparation of the report, Satcher convened a listening session in December 2000 and
held a public comment period to gather ideas from clinicians, researchers, consumers and
advocates. The sessions generated a number of community-based strategies that were
subsequently reviewed for their proven scientific effectiveness.
The strategies include:
- Ensure daily, quality physical education for all school grades. Currently, only one
state in the country-Illinois-requires physical education for grades K-12, while only
about 1 in 4 teen-agers nationwide take part in some form of physical education.
- Ensure that more food options that are low in fat and calories, as well as fruits,
vegetables, whole grains, and low-fat or non-fat dairy products, are available on school
campuses and at school events.
- Make community facilities available for physical activity for all people, including on
the weekends.
- Create more opportunities for physical activity at work sites.
- Reduce time spent watching television and in other sedentary behaviors. In 1999, 43
percent of high-school students reported watching two hours of television or more a day.
- Educate all expectant parents about the benefits of breast-feeding. Studies indicate
breast-fed infants may be less likely to become overweight as they grow older.
- Change the perception of obesity so that health becomes the chief concern, not personal
appearance.
Increase research on the behavioral and biological causes of overweight and obesity.
Direct research toward prevention and treatment, and toward ethnic/racial health
disparities.
Educate health-care providers and students in health professions on the prevention and
treatment of overweight and obesity across the life span.
The Surgeon General's Call to Action to Prevent and Decrease Overweight and Obesity
is available at:
www.surgeongeneral.gov/topics/obesity.
Homicide Risk Among Infants
- Homicide is the 15th leading cause of infant death in the United States. The risk of
homicide is greater in infancy than in any other year of childhood before age 17.
- Infants are at greatest risk for homicide during the first week of infancy and the first
day of life.
- Among homicides during the first week of life, 82.6% occurred on the day of birth.
- The homicide rate on the first day of life was more than ten times greater than the rate
during any other time of life.
- Among homicides on the first day of life, previous work has shown that 95% of victims
are not born in a hospital.
- The second highest peak in risk for infant homicide occurs during the eighth week of
life and may be due to a caregiver's reaction to an infant's persistent crying. Infant
crying duration peaks at six to eight weeks of age.
- Among homicides during the first week of life, 89% of perpetrators are female, usually
the mother. Mothers who kill their infants are more likely to be adolescents and have a
history of mental illness.
-
Teens Still Exposed to Tobacco Ads
Despite Advertising Restrictions
Despite restrictions imposed on tobacco advertising, young people are frequently
exposed to high levels of tobacco promotion in retail stores, according to a new study
released today by the Centers for Disease Control and Prevention. The study found that
more than 90 percent of retail stores that sell tobacco products had some form of tobacco
advertising including interior and exterior advertisements; self-service pack placement;
multi-pack discounts; and tobacco-branded functional objects such as shopping carts,
counter mats, or tobacco vending machines.
Overall, the report concludes that convenience, convenience/gas, and liquor stores were
most likely to have "tobacco-friendly" environments where patrons would be
highly exposed to tobacco advertisement, promotions, and tobacco branded objects in the
stores. The study, done in collaboration with the Robert Wood Johnson Foundation,
indicates that 75 percent of teenagers shop at convenience or convenience/gas stores once
a week or more.
"The pervasiveness of tobacco advertising in retail stores is weakening efforts to
prevent adolescent smoking" said Dr. Jeffrey Koplan, director of the CDC.
"Directly or indirectly, this highly visible advertising is encouraging a new
generation of children to take up a deadly habit."
An estimated 80 percent of retailers had interior tobacco advertisements with 22.8
percent of stores having high levels of such ads. Exterior tobacco advertisements were
observed in 58.9 percent of stores with 40.4 percent of stores having high levels of such
ads. While tobacco control signs, such as "We Card" signs, were observed in 65.8
percent of stores, only 4.1 percent had tobacco health warning signs.
The study evaluated marketing trends within retail outlets where tobacco products are
sold in 163 communities. Data collected on in-store tobacco product placement, promotions
(discounts or gifts with purchase), tobacco-branded functional objects (free items
provided to retailers such as shopping baskets and counter mats with tobacco brands on
them), exterior and interior advertisements, and tobacco control signage.
Other findings of the study include:
- Tobacco marketing expenditures increased from $6.7 billion in 1998 to $8.2 billion in
1999.
- Overall, some form of advertisement (interior or exterior) was present in 84.1 percent
of stores.
- Self-service cigarette pack placement was observed in 36.4 percent of stores.
- Multi-pack discounts were present in 25.2 percent of stores.
- 68.5 percent of stores had at least one tobacco-branded functional object (such as
shopping baskets or counter change mats).
"This study shows that tobacco advertising in retail stores is much more visible
to our youth than tobacco health warning information," said Rosemarie Henson, head of
the CDC's smoking and health program. "Public health efforts need to include
strategies to decrease youth exposure to tobacco products and tobacco advertising in
retail stores where they shop, and to increase youth awareness of the terrible health
consequences of using these products."
-
Court Shuts Down Website Selling Bogus Domain Names ".USA,"
".BRIT,"
Deceptively Marketed as Useable
An operation that used deceptive spam messages and appeals
to patriotism to sell Web addresses that don't work, including ".usa," has been
shut down by a U. S. District Court at the request of the Federal Trade Commission. The
court's action ensures that the defendants will not be able to reemerge by registering the
same domain names offshore. The court also ordered an asset freeze to preserve money for
consumer redress. Officials from the United Kingdom's Office of Fair Trading have been
assisting the FTC on the issue of domain name sales and are investigating such activities
in the U.K.
According to the FTC, the bogus businesses sold domain
names ending with suffixes such as ".brit," and ".bet ." After
September 11, the companies launched an aggressive spam campaign in the United States to
advertise domain names ending in ".usa." Subject lines in their e-mail read,
"Be Patriotic! Register .USA Domains." The text of the e-mail said:
"The latest domain name extension has arrived .USA!!!
It's the fresh, new, exciting web address that is taking the world by storm. Who wants to
be .com when you can now be .USA. Register your .USA domain name today exclusively at:
http://www.dotusa.com."
The hyperlink connected consumers to a Web site where they were offered the advertised
domain names for $59 each. The FTC alleges that the companies are not accredited domain
name registrars, that the ".usa" domain names are not usable on the Internet,
and that they probably never will be useable. In papers filed with the court, the agency
said that many consumers had purchased multiple bogus domain names, and the defendants
likely pocketed more than $1 million from their illegal scheme in less than a year.
"These spam scammers conned consumers in two ways," said J. Howard Beales,
III, Director of the FTC's Bureau of Consumer Protection. "They sent deceptive spam,
and they sold worthless web addresses from their Web sites. By closing down this operation
we're sending a strong signal: We will not tolerate deceptive spam."
The FTC alleges that the companies violated federal law by failing to disclose on their
Web sites that the domain names they were selling were not useable on the Internet, and by
sending the deceptive spam. The FTC has asked the court to permanently bar the operation
from deceptively selling the domain names and to order consumer redress. The defendants'
Web site domain names are registered with U. S. companies. The defendants will be
prevented from reestablishing the same domain names in another country because the domain
names have been suspended by court order. The FTC complaint names TLD Network Ltd.,
Quantum Management (GB) Ltd., TBS Industries Ltd., Thomas Goolnik, and Edward Harris
Goolnik of Finchley Road, London, England.
-
JUSTICE ENFORCEMENT, FBI, ON WHITE- COLLAR CRIME
The Federal Bureau of Investigation today released The Measurement of
White-Collar Crime Using Uniform Crime Reporting (UCR) Data, a study in the National
Incident-Based Reporting System (NIBRS) Publication Series. Defined as ". . . a crime
committed by a person of respectability and high social status in the course of his
occupation," white-collar crime extracted from NIBRS data accounts for 4 percent of
crime reported. Four percent of all arrestees reported in NIBRS were individuals arrested
for bad check offenses. The majority of white-collar crime offenders have had contact with
their victims and are typically white males aged late-twenties to early-thirties.
Computer crime, or technocrime, can be extracted in NIBRS by the data
element that notes the offender was suspected of using a computer or computer equipment to
perpetrate the crime. NIBRS data demonstrate that white-collar crime comprises 42 percent
of the offenses committed with a computer. Of those offenses, the crime of larceny-theft
accounts for the largest proportion. (See figure above.)
White-collar crime, on average, accounts for a greater dollar loss per incident when
compared to other property crime incidents. The majority of white-collar crime incidents,
with the exception of wire fraud, occur within public spaces.
Unique to NIBRS is the ability to capture information on nonperson entities that are
victimized by crime. This is particularly useful when considering white-collar crime,
where NIBRS data show that businesses are just as likely as individuals to fall victim.
In contrast to the limited data previously available on the topic of white-collar crime,
NIBRS provides information on incidents, offenses, victims, and arrestees for five
separate types of fraud, bribery, counterfeiting/forgery, embezzlement, and other offenses
that in combination could constitute white-collar crime. (See figure below.)
-
FDA APPROVES FIRST NUCLEIC ACID TEST (NAT) SYSTEM
TO SCREEN WHOLE BLOOD DONORS FOR INFECTIONS WITH HUMAN IMMUNODEFICIENCY VIRUS (HIV) AND
HEPATITIS C VIRUS (HCV)
The Food and Drug Administration has licensed the first nucleic acid test (NAT) system
intended for screening donors of whole blood and blood components intended for use in
transfusion. This test system can simultaneously detect the presence of HIV and HCV in
blood using a semi-automated system and is expected to further ensure the safety of whole
blood and blood components, including fresh plasma, red cells and platelets, by permitting
earlier detection of HIV and HCV infections in donors.
FDA also recently licensed the first NAT system for screening donors of plasma for the
specific use in products that will be further manufactured, such as clotting factors and
immune globulins.
The approved test system was developed by Gen-Probe Inc., San Diego, Calif. and will be
distributed by Chiron Corporation, Emeryville, Calif.
Blood donors have been tested for evidence of HIV infection since 1985 and for evidence
of HCV infection since 1990. Although increasingly sensitive tests for detection of HIV
and HCV antibodies and HIV antigen were implemented during the past decade, in rare
instances infections in donors have been missed.
The NAT system is capable of detecting more infectious donations than current tests
because it detects viral genes rather than antibodies or antigens (proteins from the
virus). Detection of viral genes permits detection earlier in the infection since the
appearance of antibodies requires time for the donor to develop an immune response, and
since detection of antigens requires time for a higher level of virus to appear in the
bloodstream.
This new technology detects very small amounts of genetic material by copying the genes
numerous times, resulting in a billion-fold amplification of the target gene. The approved
test system can detect ribonucleic acid (RNA) from HIV-1 and HCV when tested in pools of
16 samples obtained from multiple donors. In a less automated format, it can also be used
to test individual samples from whole blood collections. If a test pool is positive for
either virus, the individual donation suspected of containing a virus can be identified
and not transfused. The donor can be deferred from donating blood and notified.
Currently, donors of blood and plasma are tested for antibodies to HCV, antibodies to
HIV and HIV-1 antigens, which are the virus’s own proteins. However, there is still a
“window period” during which a donor can be infected, but have negative
screening tests. With the use of NAT for HCV, the window period is reduced by
approximately 57 days (from an average of 82 days to 25 days). For HIV-1, the average
window period with antibody is 22 days. This window period is reduced approximately to 16
days with antigen testing and to 12 days with NAT.
In nation-wide clinical trials performed to support the approval of the test on pools,
a total of 7 HIV-1 positive and 88 HCV positive donations were detected in more than 20
million donations tested confirming the effectiveness of the test. The NAT system using
pools was evaluated at eight volunteer blood donor sites while NAT for use with individual
donations used data from U.S. military blood donor sites.
The use of the licensed test will allow blood banks that implement it to discontinue
antigen testing, although blood donations will continue to be tested by antibody tests.
FDA plans to issue guidance on the use of NAT in the near future.
Since 1997, FDA has encouraged the large-scale study of NAT through the use of
experimental protocols. More than one test system is under development. Most of the
nation’s blood establishments now participate in these experimental protocols. The
Gen-Probe NAT system is the first to be approved to screen donors of whole blood and blood
components intended for use in transfusion.
- COMMUNITY WATER FLUORIDATION NOW REACHES NEARLY
TWO-THIRDS OF U.S. POPULATION
Nearly two-thirds of U.S. residents who receive water from public water systems now
receive fluoridated water, according to an article released today by the Centers for
Disease Control and Prevention (CDC).
The article, "Populations Receiving Optimally Fluoridated Public Drinking Water --
United States, 2000," provides the most recent information on the status of water
fluoridation by state. Between 1992 and 2000, the percent of the U.S. population receiving
fluoridated water increased from 62.1 percent to 65.8 percent, bringing the total U.S.
population receiving fluoridated water to approximately 162 million.
Fluoride, a naturally occurring element in the environment, is known to be effective in
preventing tooth decay in children and adults. Over the past several decades, fluoridation
has played an important role in the dramatic reduction of tooth decay and has been
identified by CDC as one of
the 10 greatest public health achievements in the twentieth century. However, tooth decay
remains the most prevalent chronic infectious disease of childhood; 80 percent of all
children have had dental decay by the time they are 18 years of age. Recent estimates of
effectiveness indicate that water fluoridation reduces tooth decay among children by 18
percent to 40 percent.
The importance of fluoridation for reducing tooth decay was highlighted in the first
Surgeon General's report on oral health
(http://www.surgeongeneral.gov/library/oralhealth/) issued in May 2000.
The Healthy People 2010 national health initiative set an objective for 75 percent of the
U.S. population on public water systems to receive fluoridated water. Between 1992 and
2000, five additional states (Delaware, Maine, Missouri, Nebraska and Virginia) achieved
the Healthy People objective, and Oklahoma was close (74.6 percent) to achieving this
goal. Twenty-six states and the District of Columbia have now met this objective.
State-specific percentages range from 2 percent to 100 percent of persons on public water
systems that receive optimally fluoridated water.
"Water fluoridation is the most equitable and cost-effective means we have of
delivering fluoride to all members of most communities," said Dr. William R. Maas,
director of CDC's Oral Health Program. "While several states, such as California, New
Hampshire and Nevada have made substantial progress, there is considerable need as well as
opportunity for additional improvement, particularly in the 24 states that have not yet
met the objective of having at least 75 percent of their populations on public water
systems receiving fluoridated water."
The fluoridation update appears in today's Morbidity and Mortality Weekly Report, which
can be viewed or downloaded at www.cdc.gov/mmwr/
preview/mmwrhtml/mm5107a2.htm. Other information on fluoridation and oral health is
available on-line through the oral health web site: www.cdc.gov/nccdphp/oh or by calling
770-488-5131 or 770-488-6054.
CDC protects people's health and safety by preventing and controlling diseases and
injuries; enhances health decisions by providing credible information on critical health
issues; and promotes healthy living through strong partnerships with local, national, and
international organizations.
- FDA ANNOUNCES FOODS ADVISORY COMMITTEE TO MEET ON
METHYL MERCURY IN SEAFOOD
The Food and Drug Administration (FDA) today announced that it will soon schedule a
meeting of its Foods Advisory Committee to review issues surrounding methyl mercury in
commercial seafood. This review will include a re-examination of FDA's most recent
Consumer Advisory, issued in January 2001 and revised in March 2001, for pregnant women
and women of child-bearing age who may become pregnant.
The advisory recommended that these women should avoid eating the four fish species with
the highest levels of methyl mercury: shark, swordfish, king mackerel, and tile fish. It
concluded that these women could safely eat 12 ounces per week of a variety of other fish,
with the emphasis on choosing a variety of different species.
At that time, FDA set forth its rationale for this decision in a formal, publicly
available document, "Rationale for Issuance of Revised Advisory on Methyl Mercury and
Fish Consumption." This document is available on FDA's web site at
http://www.cfsan.fda.gov/~acrobat/hgadv4.pdf.
A recent report by the Environmental Working Group calls into question the basis for FDA's
Consumer Advisory and the way in which FDA reached its conclusions on methyl mercury in
seafood for this group of women.
FDA stands behind the process that led to its current Consumer Advisory on this subject,
as well as the science that supports that advisory. In reaching its conclusions about
methyl mercury in fish, FDA met with a broad range of interested parties, including
consumer groups, health professionals, industry, and state public health officials.
-
Protein Patterns May Identify Ovarian Cancer
Scientists from the Food and Drug Administration (FDA) and the National Cancer
Institute (NCI) report today, in a special fast-tracked release in
The Lancet*,
that patterns of proteins found in patients' blood serum may reflect the presence of
disease. In the study, scientists used serum proteins to detect ovarian cancer, even at
early stages. They report that this new diagnostic concept is potentially applicable to
any type of disease.
Using a test that can be completed in 30 minutes using blood that can be obtained from
a finger stick, researchers were able to differentiate between serum samples taken from
patients with ovarian cancer and those from unaffected individuals.
The research, a joint effort between the FDA/NCI Clinical Proteomics Program and
Correlogic Systems Inc., unites two exciting disciplines: proteomics - the study of the
proteins inside cells - and artificial intelligence computer programs.
The diagnostic test relied on software that is able to detect patterns of key proteins
in the blood. Using a sophisticated artificial intelligence computer program developed by
Correlogic, scientists were able to "train" the computer to distinguish between
patterns of small proteins found in the blood of cancer patients vs. control samples. The
artificial intelligence program identified a pattern consisting of only a handful of
proteins, among thousands, that could be used to distinguish between women with ovarian
cancer and women with non-cancerous conditions.
"The idea that rather than a single biomarker, an entire pattern of proteins
contains important diagnostic information, is an exciting new paradigm," said J. Carl
Barrett, Ph.D., director of the NCI's Center for Cancer Research, which oversees the
proteomics program.
The scientists first used serum samples from known cancer patients and unaffected
individuals to establish proteomic patterns which were present at different levels in the
two groups. Once these patterns were identified, the researchers compared them with the
patterns of the same proteins in serum samples from other patients with and without
cancer. The researchers correctly identified 50 out of 50 cancers and 63 of 66 non-cancer
samples.
The researchers analyzed the serum proteins with mass spectroscopy, a technique used to
sort proteins and other molecules based on their weight and electrical charge. The
identity of the key proteins and the role they may play in cancer is unknown, but being
investigated.
An important finding was the ability to correctly identify, in a small sample of
patients, all stage I ovarian cancer cases. Currently, more than 80 percent of ovarian
cancer patients are diagnosed at a late clinical stage and have a 20 percent or less
chance of survival at five years. In contrast, the 20 percent of women diagnosed with
early-stage disease have an excellent prognosis, with over 95 percent alive at five years
after diagnosis. The results of this study indicate that proteomic technology may help
clinicians diagnose the disease much earlier than current methods.
The authors of the paper caution that further study is needed to confirm the
sensitivity and accuracy of this technique as a diagnostic tool. They hope that by
combining the proteomic approach with other methods of ovarian cancer diagnosis, such as
ultrasound, its accuracy can be further improved.
"Simple, accurate, and non-invasive methods for early detection of epithelial
ovarian cancer may improve quality of life and survival and reduce unnecessary suffering
for patients," said Kathryn Zoon, director of the Center for Biologics Evaluation and
Research (CBER) at the FDA. The majority of the individuals included in the study had an
increased risk of ovarian cancer, due to a family history of the disease, or mutations in
BRCA1 or BRCA2 genes, which increase risk for both breast and ovarian cancers. Researchers
on the study from Northwestern University Medical School, Chicago, considered it important
to test the method in this population, as these are the women most in need of effective
screening options.
"The most important next goal is validating the promise of these results in large,
multi-institutional trials. Early detection means we can treat the cancer before it has
spread," said Lance Liotta, M.D., Ph.D., the senior investigator on the study from
the NCI's Center for Cancer Research. Such trials are under way at the NCI, evaluating
proteomics both alone and in combination with current screening methods for ovarian
cancer.
"We're particularly excited about the potential of this technique to diagnose
additional types of diseases. It may also be able to provide an early warning of impending
toxicity," said the first author of the study, Emanuel Petricoin, Ph.D., of the FDA's
CBER.
USFDA APPROVES NEW WEARABLE DEFIBRILLATOR
FOR SERIOUSLY ILL HEART PATIENTS
The Food and Drug Administration today approved a vest-like medical device that is worn
under clothing to monitor and treat abnormal heart rhythms in people at risk of dying from
sudden cardiac arrest.
The product, made by Lifecor, Inc., of Pittsburgh, Pa., is the first cardioverter
defibrillator that can be worn outside the body, rather than implanted in the chest.
The device is a programmable system that senses heart function and automatically
delivers an electrical shock when needed to restore normal heart rhythm.
Until now, people who needed a cardioverter defibrillator had to have it surgically
implanted into their chest.
"Today's approval represents a significant advance in defibrillator technology. It
means patients may now opt for a wearable defibrillator if they are not suitable
candidates for an implanted defibrillator or do not want one," said FDA Acting
Principal Deputy Commissioner Bernard A. Schwetz, D.V.M., Ph.D.
The new product consists of an electrode belt assembly that is worn around the chest,
touching the skin. It is connected to a monitor, with an alarm, that is worn in a holster
at the waist. This entire device assembly is worn continuously 24 hours a day, except when
the wearer is bathing or showering.
The device continuously monitors the patient's heart to detect life-threatening
abnormal heart rhythms. Typically, once a week the physician will want the patient to
connect the monitor to an external modem and send the data over the phone to the
physician's computer for his review.
The defibrillator detects abnormal heart rhythms by sensing the heart's electrical
activity on the surface of the chest. If a life-threatening rhythm is detected and the
person loses consciousness, the device delivers an electrical shock to restore normal
rhythm.
FDA approved the wearable defibrillator based on a review of laboratory and animal
tests and clinical studies of safety and effectiveness conducted by Lifecor.
Some 289 heart patients at 16 medical centers in the United States and Europe were
fitted with the defibrillator vest. All were either awaiting heart transplants or had
recently had a heart attack or a coronary bypass operation. The patients wore the
defibrillator for an average of 20 hours a day for approximately three months.
The wearable defibrillator was 71 percent successful in treating sudden cardiac arrest
episodes compared to 25 percent success for patients calling 911. It successfully detected
and treated five episodes of sudden cardiac arrest, and detected but was unable to treat
two other episodes. The two failures to treat resulted because the patients had
incorrectly assembled the electrodes in the vest. Lifecor subsequently changed the design
of the garment to make it more user-friendly.
Two percent of patients experienced an unnecessary shock from the wearable device,
compared to 2.3 percent false shocks per patient-month received by patients with an
implantable defibrillator. Lifecor subsequently modified the device to further reduce the
rate of unnecessary shocks.
The most frequent side effect was a temporary skin rash, experienced by 5.9 percent of
study patients.
PRO-ATHLETES
HELP CDC LAUNCH TOBACCO-FREE SPORTS PLAYBOOK
The Sports Playbook profiles many of the world's top athletes and sports figures and is
designed to help communities throughout the country develop and implement programs that
promote sports as a healthy alternative to tobacco use. It is part of the World Health
Organization's (WHO) Tobacco-Free Sports Initiative.
"Sports activities are a great way to reach our nation's young people with
information about how to make important health decisions–specifically, those
decisions related to tobacco use, physical activity, and good nutrition," said CDC
Director Dr. Jeffrey P. Koplan.
Research shows that students who participate in interscholastic sports are less likely to
be heavy smokers while students who play at lease one sport are 40 percent less likely to
be regular smokers and 50 percent less likely to be heavy smokers. Almost 90 percent of
adult smokers began smoking before the age of 18. Each day, more than 3,000 kids become
regular smokers and roughly one-third of them will eventually die from tobacco-related
disease.
"By getting kids involved in sports, you are reducing the amount of unsupervised time
they can spend doing things like using tobacco," Jackson said. "I am very proud
to have the opportunity to support the Sports Playbook."
The Sports Playbook offers guidance and real-world examples of how coaches, teachers,
school leaders, and community leaders can launch successful tobacco control initiatives
and profiles many of the world's top athletes and sports figures in illustrating the wide
variety of sports available to youth. "It is a step-by-step game plan for
incorporating sports in tobacco-free activities," Koplan said.
For more information about this initiative or other tobacco control programs, call CDC's
Office on Smoking and Health at 770-488-5747 or visit the Tobacco Information and
Prevention Source at www.cdc.gov/tobacco/
CALIFORNIA DEFENDANTS TO PROVIDE REDRESS FOR CHARGING
CONSUMERS A"CANCELLATION" FEE FOR DELAYED SHIPMENTS
Commission Also Alleged Other
Violations of its Mail or Telephone Order Merchandise Rule
The Federal Trade Commission today announced a consent decree with a California-based
aftermarket automobile accessories seller resolving charges of violating the FTC's Mail or
Telephone Order Merchandise Rule by making unsubstantiated shipment representations and
failing to provide consumers with timely and complete delay notices. The Commission also
alleged that the defendants violated the Rule by substituting merchandise that was
materially different from what consumers ordered without the consumers' prior consent, and
by charging consumers a 20 percent "cancellation" fee when consumers cancelled
because of delayed shipment.
Under the terms of the consent decree, filed by the Department of Justice (DOJ) on the
FTC's behalf, the defendants, Charles Smith, Damian Smith, and Kymberli Smith, doing
business as Salesco, will pay a $15,000 civil penalty, will provide redress to consumers
whose refunds were discounted in violation of the Rule, and will be required to comply
with the Rule in the future.
"The Mail or Telephone Order Merchandise Rule guarantees that consumers get what
they ordered -- and get it when it was promised," said FTC's Bureau of Consumer
Protection Director Howard Beales. "The FTC expects catalog, telephone, and Internet
retailers to deliver the goods as required by law, not only because it's good business,
but because it enhances consumer confidence."
An unincorporated business based in San Dimas, California, since 1995, Salesco has sold
automobile accessories including audio equipment, seat belt extensions, canopies, chrome
plated wheels, dashboards, seats, carpet kits, and car covers to consumers throughout the
United States via mail order, telephone, and the Internet. The FTC's Mail or Telephone
Order Merchandise Rule covers - in addition to orders by mail - orders by any "direct
or indirect" use of the telephone, including orders by Facsimile or the Internet.
The Commission's Complaint
According to the Commission's complaint, the defendants violated the FTC's Mail or
Telephone Order Merchandise Rule over a two-and-a-half year period in numerous
transactions by making unsubstantiated shipment representations and failing to provide
timely and complete delay notices to consumers. The defendants allegedly failed to keep
records demonstrating Rule compliance, including inventory records and records relating to
shipment. When shipment delays occurred, they often failed to notify consumers of the
delay. In the instances in which they did notify consumers of delays, the FTC alleges, the
notices failed to include a revised shipment date or the statement that the consumers
could cancel and obtain prompt, full refunds, as required by the Rule.
The FTC's complaint alleged that when consumers contacted the company in response to
Salesco's Internet advertising, the defendants allegedly told them that the advertised
merchandise was "in stock" and would ship within a certain time. In fact, the
complaint alleged, the merchandise was often not in stock. On such occasions, defendants
would, without the consumers' prior consent, ship items that were materially different
from what they had ordered. Consumers dissatisfied with these substitutions had to pay to
return them.
On other occasions, the defendants charged consumers who cancelled because shipment had
been delayed beyond the promised shipment time a 20 percent "cancellation" fee.
The complaint alleges that the practice of unilaterally substituting merchandise that is
materially different from the merchandise ordered by consumers by mail or telephone, and
the practice of failing to provide full refunds when consumers cancel their mail or
telephone orders because of delayed shipment, both violate the FTC's Mail or Telephone
Order Merchandise Rule.
The Consent Decree
The settlement includes a $200,000 civil penalty against the defendants, all but
$15,000 of which will be suspended due to their financial situation. In addition, the
defendants will be required to compile (from their business records and other information)
a list of consumers whose refunds were discounted and to provide them with full refunds.
These redress activities must subsequently be reported to Commission staff.
The settlement enjoins the defendants from failing to comply with the Rule in the
future, including failing to: 1) have a reasonable basis for their shipment
representations; 2) provide timely and compliant notification of delays; and 3) provide
full and prompt refunds in all situations in which the Rule requires a refund. It also
enjoins the defendants from substituting materially different mail or telephone order
merchandise without the consumer's prior express consent. In situations in which consumers
authorize the defendants to ship materially different merchandise, the defendants will be
required to offer them the right to return the merchandise within a reasonable time at the
defendants' expense.
The consent decree requires the defendants to keep specific detailed records of their
systems and procedures for complying with the Mail or Telephone Order Rule. Finally, the
consent contains other recordkeeping, reporting and compliance requirements to which the
defendants must adhere.
The Commission vote to forward the complaint and consent decree to the Department of
Justice for filing was 5-0. It was filed in the Federal District Court for the Central
District of California. FTC staff was assisted in its investigation by the Better Business
Bureau of the Southland
MARYLAND
BUSINESSMAN SENTENCED FOR ILLEGALLY MARKETING ALOE VERA COMPOUNDS AS AIDS AND CANCER
TREATMENTS
Hoffman pleaded guilty to two felony counts of introduction of an unapproved new drug into
interstate commerce with the intent to defraud the public. Under the Federal Food, Drug,
and Cosmetic Act, it is illegal to market a drug that has not been approved by the Food
and Drug Administration (FDA) for treatment of specific illnesses.
Hoffman, doing business as T-Up, Inc., of Baltimore, Md., and Astec Biologics, Inc. of
Hanover, Pa., charged cancer patients and their families up to $18,000 for a two-week
treatment with intravenous aloe vera. He also sold bottled combinations of aloe vera and
other unapproved drugs to treat auto-immune diseases. More than 3,000 people purchased
products from Hoffman, who falsely claimed to have a doctoral degree.
This case was investigated by FDA's Office of Criminal Investigations, the Internal
Revenue Service - Criminal Investigation and the United States Postal Inspection Service,
with the assistance of the Maryland State Attorney General's Office of Consumer
Protection.
The sentence was announced by U.S. District Judge William M. Nickerson.
STRATEGIC FBI
HEADQUARTERS REORGANIZATION
Congress approved, and today the Director implemented, a restructuring
plan for Headquarters, Federal Bureau of Investigation (FBI), the first step in what will
be a phased process of reorganizing assets, modernizing and integrating new technology,
and consolidating functions. This reorganization was considered and approved by the
Attorney General's Strategic Management Council and will serve as the foundation as the
FBI redefines priorities and missions in the coming months.
This reorganization, the need for which is widely accepted within the FBI community, is
consistent with the recommendations from several studies and inquiries, and recognizes new
challenges and responsibilities. Among other things, it seeks to increase the emphasis in
counterterrorism, counterintelligence, cybercrimes, and relations with state and local law
enforcement. It also seeks to provide the vehicle for a vastly enhanced information
technology upgrade, expanded training for the FBI workforce at all levels, improved
security, and improved capabilities for FBI investigators, analysts, forensic examiners,
and other specialists.
The major elements of the first phase of the Headquarters reorganization effort include
the creation of four new Executive Assistant Director positions to oversee key FBI
functions.
The positions and their designated heads include:
* Executive Assistant Director for Criminal Investigations - To be headed by Ruben Garcia,
Jr., 23-year FBI veteran who was formerly the Assistant Director of the Criminal
Investigative Division.
* Executive Assistant Director for Counterterrorism/Counterintelligence - To be headed by
Dale L. Watson, currently the Assistant Director for the Counterterrorism Division. Mr.
Watson entered the Bureau in 1978 and has served continually in intelligence and
counterterrorism roles since 1982. In 1996, he was named the Deputy Chief of the CIA's
Counterterrorist Center at CIA Headquarters.
* Executive Assistant Director for Law Enforcement Services - To be headed by 23-year
veteran Kathleen L. McChesney. Currently the Assistant Director of the FBI Training
Division, she has served as Special Agent in Charge of the Portland, Oregon and Chicago
Field Offices.
* Executive Assistant Director for Administration - To be headed by Robert J. Chiaradio,
currently an assistant to FBI Director Robert Mueller. A veteran of the FBI since 1984,
Chiaradio was previously the Special Agent in Charge of the Tampa Field Office and the
Chief of Staff for the FBI Deputy Director.
FBI divisions and offices will realign under one of these four Executive Assistant
Directors who report through the offices of the Director/Deputy Director. This
reorganization step effectively narrows the supervisory span of control and will greatly
increase efficiency, accountability and oversight.
Two new divisions have also been created to increase emphasis on computer-facilitated
crimes and security. The Cybercrime Division will address intellectual property
investigations, as well as high tech and computer crimes. The Security Division will be
responsible for ensuring the integrity of FBI employees, contractors, visitors,
information systems, and facilities.
Also a part of this phase of reorganization is the opening of four new offices: Law
Enforcement Coordination for improving FBI coordination with state and local law
enforcement and information sharing; Chief Technology Officer reporting directly to the
Office of the Director and charged with the implementation of the ongoing critical
information technology projects; Office of Records Management whose function is the
modernization of FBI records, including management policies and processes; and the
Intelligence Office charged with enhancing analytical and intelligence capabilities,
particularly in the critical counterterrorism and counterintelligence areas.
The Investigative Services Division will be disbanded as a result of this reorganization
and its important responsibilities and assets integrated into current or newly created
components as appropriate.
Attached to this release is an expanded breakdown of the Headquarters Phase I
reorganization, an organizational chart showing the new realignments and biographical
information on the newly appointed Executive Assistant Directors.
The second phase of Headquarters reorganization, which will deal with changes at the
Divisional and Office levels of the FBI, will focus on such areas as eliminating
duplication, consolidating functions, and realigning resources.
When coupled with new hiring priorities aimed at special skill sets, workforce development
initiatives, and a particular emphasis on developing an overarching leadership climate at
every level of Bureau operations, Phase II reorganization promises measurable enhancements
in tune with new law enforcement challenges and realities.
The reorganization of FBI Headquarters is part of the Director's comprehensive plan to
address not only the new challenges of terrorism, but to modernize and streamline the
Bureau's more traditional functions so that it may better serve not only its law
enforcement partners, but the nation.
The Food and Drug Administration today approved two devices that may provide an
alternative treatment to open heart surgery for patients with two types of congenital
heart defects.
The devices, called septal occluders, are implanted in the heart by way of catheters (thin
plastic tubes) inserted into either an artery or a vein.
The two types of congenital heart defects are ventricular septal defect, a hole between
the bottom chambers of the heart, and atrial septal defect, a hole between the top
chambers of the heart. Normally these defects are corrected through open heart surgery.
The products are the Cardioseal Septal Occlusion System, made by NMT Medical, Inc., of
Boston, Mass., approved to close complex ventricular septal defects; and the Amplatzer
Septal Occluder, made by AGA Medical Corporation, of Golden Valley, Minn., approved to
close secundum atrial septal defects, those located in the mid portion of the atrial
septum.
The devices are made from either a metal frame or wire mesh and fabric. The design and
shape of the products vary, as does the exact mode of deployment.
FDA based its approval of the two products on a review of clinical studies of safety and
effectiveness conducted by the manufacturers and on the recommendation of the Circulatory
Systems Devices Panel of FDA's Medical Devices Advisory Committee.
FDA is requiring each company to continue to study its product over the next five years to
better assess the long-term safety and effectiveness of the devices.
THE "HEALTH CARE
PRESIDENT" SIGNS
RECORD FY 2002 BUDGET
For the first time in several years Congress has provided a budget for the
Food and Drug Administration over and above increases requested for the Salaries and
Expense account. The biggest impact will result from the funding for the full pay raise of
4.6%. FDA's total program level is $1.4 billion and includes full funding for the
Buildings and Facilities account as well as Prescription Drug User Fees Act and
Mammography Quality Standards Act User Fees, and the Export Certification and
Certification fund. The Salaries and Expenses Appropriation totals $1.345 billion,
including $1.2 billion for Salaries and Expenses, and $161.716 million for PDUFA. This
budget reflects the commitment of the Administration and the Congress to continue
strengthening the public health protection by focusing on urgent public health hazards. A
breakdown of the increases follows:
- $45.2 million to meet mandated cost-of-living and pay-related increases for FDA's
employees. In the last eight years, FDA has had to absorb $284 million in unfunded pay
raises and other inflationary costs;
- $15 million to protect consumers against the new variant Creutzfeldt- Jakob Disease, a
fatal illness associated with consumption of meat from cows with Bovine Spongiform
Encephalopathy (BSE). The funds were provided to keep BSE, the "Mad Cow
Disease," out of the United States;.
- $10.3 million to prevent substandard food and health care products from reaching the
U.S. market by increasing plant inspections and expanding surveillance of regulated
imports;
- $9.4 million to significantly upgrade food safety by expanding the highly successful
Food Safety Initiative beyond microbiological contaminants to cover chemical and physical
food hazards;
- $10 million to safeguard patients against adverse events associated with the use of
drugs, biological agents and medical devices by improving FDA's system for monitoring
marketed products;
- $10 million to protect the human subjects and research data in clinical trials by
increasing FDA's inspections;
- $10.1 million to enhance FDA's scientific potential and operational efficiency through
infrastructure improvements. This includes funding for the development of an advanced
financial management system, the completion of a new laboratory/office complex in Los
Angeles, and the initial move of a FDA center to the White Oak campus;
- $13.1 million for current low user fees, including increases for Prescription Drug User
Fees Act and Mammography Quality Standards Act fees, Certification fund and Export fund.
- Congress also provided $10.5 million in additional funding without impacting the
President's budget request. Earmarks include $ 3.0 million for Dietary Supplements; $2.5
million for generic drug review and education; $1.0 million for Orphan Drug Grants and,
$0.5 million for a gene therapy data base; $3.0 million for activities related to
antibiotic drugs; and, $0.5 million to develop a database focused on woman’s health
issues.
These resources will allow FDA to continue its important role in effective health care
delivery and ensure continued consumer confidence in the products we regulate.
David N. Rahni, Ph.D is a Professor of Analytical Chemistry and
Adjunct Professor, Environmental Law and Dermatology (NYMC).
David has been awarded an honorary fellowship in the Academy for
Justice Through Science. Read as "David takes on the Goliath" of
germ/bio for 2001 by clicking on the link above or
here now".
FBI ASKS CAN YOU HELP IDENTIFY THE ANTHRAX LETTERS?
Today the FBI is releasing linguistic and behavioral assessments of the
person responsible for mailing anthrax-laden letters on September 18 and October 9, 2001.
We ask the American public to study these assessments and reflect on whether someone of
their acquaintance might fit the profile. The safety of the American people is at stake.
If you have credible information that might help identify this person, please contact
1-800-CRIMETV (274-6388), use www.ifcc.fbi.gov,
or call your local FBI field office.
EVIDENCE DESCRIPTION
Letter 1
One page, hand-printed letter
Transmittal envelope, also similarly hand printed
Addressed to "NBC TV – Tom Brokaw" – No return address
Postmarked Trenton, NJ 09/18/2001 (Tues.)
Letter 2
One page, hand-printed letter
Transmittal envelope, also similarly hand printed
Addressed to "NY Post" – No return address
Postmarked Trenton, NJ 09/18/2001 (Tues.)
Letter 3
One page, hand-printed letter
Transmittal envelope, also similarly hand printed
Addressed to "Senator Daschle – 509 Hart Senate Office Building"
Return address – "4th Grade, Greendale School, Franklin Park, NJ"
Return address zip code – "08852"
Postmarked Trenton, NJ 10/09/2001 (Tues.)
LINGUISTIC ASSESSMENT
It is highly probable, bordering on certainty, that all three letters were authored by the
same person. Letters 1 and 2 are identical copies. Letter 3, however, contains a somewhat
different message than the other letters. The Anthrax utilized in Letter 3 was much more
refined, more potent, and more easily disbursed than letters 1 and 2.
In the past, the public has helped the FBI solve high profile investigations that
involved writings by coming forward to identify the author, either by how he wrote or by
what he wrote. We are asking for the public's help here again in the same way.
While the text in these letters is limited, there are certain distinctive
characteristics in the author's writing style. These same characteristics may be evident
in other letters, greeting cards, or envelopes this person has written. We hope someone
has received correspondence from this person and will recognize some of these
characteristics.
The characteristics include:
1. The author uses dashes ("-") in the writing of the date
"09-11-01." Many people use the slash ("/") to separate the
day/month/year.
2. In writing the number one, the author chooses to use a formalized, more detailed
version. He writes it as "1" instead of the simple vertical line.
3. The author uses the words "can not," when many people prefer to spell it
as one word, "cannot."
4. The author writes in all upper case block-style letters. However, the first letter
of the first word of each sentence is written in slightly larger upper case lettering.
Also, the first letter of all proper nouns (like names) is slightly larger. This is
apparently the author's way of indicating a word should be capitalized in upper case
lettering. For whatever reason, he may not be comfortable or practiced in writing in lower
case lettering.
5. The names and address on each envelope are noticeably tilted on a downward slant
from left to right. This may be a characteristic seen on other envelopes he has sent.
6. The envelopes are of the pre-stamped variety, the stamps denoting 34 cents, which are
normally available directly from the post office. They are not the traditional business
size envelopes, but the smaller size measuring approximately 6 1/4" x 3 ˝".
BEHAVIORAL ASSESSMENT
Based on the selection of Anthrax as the "weapon" of choice by this
individual, the offender:
• is likely an adult male.
• if employed, is likely to be in a position requiring little contact with the
public, or other employees. He may work in a laboratory. He is apparently comfortable
working with an extremely hazardous material. He probably has a scientific background to
some extent, or at least a strong interest in science.
• has likely taken appropriate protective steps to ensure his own safety, which may
include the use of an Anthrax vaccination or antibiotics.
• has access to a source of Anthrax and possesses knowledge and expertise to
refine it.
• possesses or has access to some laboratory equipment; i.e., microscope,
glassware, centrifuge, etc.
• has exhibited an organized, rational thought process in furtherance of his
criminal behavior.
• has a familiarity, direct or indirect, with the Trenton, NJ, metropolitan area;
however, this does not necessarily mean he currently lives in the Trenton, NJ, area.. He
is comfortable traveling in and around this locale.
• did not select victims randomly. He made an effort to identify the correct
address, including zip code, of each victim and used sufficient postage to ensure proper
delivery of the letters. The offender deliberately "selected" NBC News, the New
York Post, and the office of Senator Tom Daschle as the targeted victims (and possibly AMI
in Florida). These targets are probably very important to the offender. They may have been
the focus of previous expressions of contempt which may have been communicated to others,
or observed by others.
• is a non-confrontational person, at least in his public life. He lacks the
personal skills necessary to confront others. He chooses to confront his problems
"long distance" and not face-to-face. He may hold grudges for a long time,
vowing that he will get even with "them" one day. There are probably other,
earlier examples of this type of behavior. While these earlier incidents were not actual
Anthrax mailings, he may have chosen to anonymously harass other individuals or entities
that he perceived as having wronged him. He may also have chosen to utilize the mail on
those occasions.
• prefers being by himself more often than not. If he is involved in a personal
relationship it will likely be of a self serving nature.
Pre-Offense Behavior
• Following the events of September 11, 2001, this person may have become mission
oriented in his desire to undertake these Anthrax mailings. He may have become more
secretive and exhibited an unusual pattern of activity. Additionally, he may have
displayed a passive disinterest in the events which otherwise captivated the Nation. He
also may have started taking antibiotics unexpectedly.
Post-Offense Behavior
• He may have exhibited significant behavioral changes at various critical periods
of time throughout the course of the Anthrax mailings and related media coverage. These
may include the following;
1. Altered physical appearance.
2. Pronounced anxiety.
3. Atypical media interest.
4. Noticeable mood swings.
5. More withdrawn.
6. Unusual level of preoccupation.
7. Unusual absenteeism.
8. Altered sleeping and/or eating habits.
These post-offense behaviors would have been most noticeable during critical times,
including but not limited to: the mailing of the letters (09/18/01 and 10/09/01), the
death of first Anthrax victim, media reports of each anthrax incident, and especially the
deaths and illnesses of non-targeted victims.
AGAIN, IF YOU HAVE CREDIBLE INFORMATION THAT MIGHT HELP IDENTIFY THIS PERSON, PLEASE
CONTACT THE FBI IMMEDIATELY AT 1-800-CRIMETV
(274-6388), AT WWW.IFCC.FBI.GOV,
OR BY CALLING YOUR LOCAL FBI FIELD OFFICE. InfoJustice
CDC Prepares Teams to Respond to Possible Smallpox
Outbreak
CDC is taking steps to protect the public's health in case of an intentional release of
smallpox. Teams – which include physicians, epidemiologists, laboratorians –
have been vaccinated against smallpox and are attending readiness-training at CDC to
identify and contain smallpox outbreaks. Each team could be immediately dispatched from
CDC to assist local and state health departments if a case of this contagious disease is
suspected. Smallpox is difficult to recognize because it was eradicated from the world
more than 20 years ago. This is part of CDC's ongoing public health emergency response
efforts. For more information, visit: http://www.bt.cdc.gov/DocumentsApp/ImprovingBioDefense/
ImprovingBioDefense.asp.
CDC confirmed cases of anthrax
Summary of Local, State, and Federal Confirmed Human Cases and Exposures
| Confirmed |
2 |
5 |
5 |
5 |
17 |
| Cutaneous |
0 |
4 |
3 |
0 |
|
| Inhalational |
2 |
1 |
2 |
5 |
|
| Suspect |
0 |
3 |
2 |
0 |
5 |
| Cutaneous |
0 |
3 |
2 |
0 |
|
| Inhalational |
0 |
0 |
0 |
0 |
|
| Total Cases |
|
|
|
|
22 |
There have been 4 deaths associated with inhalational anthrax.
CDC confirmed cases are based on a rigorous case definition, which was published in
CDC’s Morbidity and Mortality Weekly Report (MMWR) on October 19, 2001. The
MMWR is available on-line at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5041a1.htm.
CDC defines a confirmed case of anthrax as 1) a clinically compatible case of
cutaneous, inhalational, or gastrointestinal illness that is laboratory confirmed by
isolation of B. anthracis from an affected tissue or site or 2) other laboratory
evidence of B. anthracis infection based on at least two supportive laboratory
tests. CDC defines a suspect case as 1) a clinically compatible case of illness
without isolation of B. anthracis and no alternative diagnosis, but with laboratory
evidence of B. anthracis by one supportive laboratory test or 2) a clinically
compatible case of anthrax epidemiologically linked to a confirmed environmental exposure,
but without corroborative laboratory evidence of B. anthracis infection.
CDC Telebriefings / Information
Telebriefings regarding CDC activities and the anthrax investigations will be conducted
during the entire month of November, on Monday through Friday, from Noon - 12:45 PM, EST.
The toll-free number for these briefings is 1-866-254-5942. For the latest update
on CDC activities and on-going anthrax investigations visit www.bt.cdc.gov or www.cdc.gov/od/oc/media.
CDC UDATE:
CDC confirmed cases of anthrax
Summary of Local, State, and Federal Confirmed Human Cases and Exposures
| Confirmed |
2 |
4 |
5 |
5 |
16 |
| Cutaneous |
0 |
3 |
3 |
0 |
|
| Inhalational |
2 |
1 |
2 |
5 |
|
| Suspect |
0 |
4 |
2 |
0 |
6 |
| Cutaneous |
0 |
4 |
2 |
0 |
|
| Inhalational |
0 |
0 |
0 |
0 |
|
| Total Cases |
|
|
|
|
22 |
There have been 4
deaths associated with inhalational anthrax.
CDC confirmed cases
are based on a rigorous case definition which was published in CDC’s Morbidity and
Mortality Weekly Report (MMWR) on October 19, 2001.
The MMWR is available on-line at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5041a1.htm.
CDC defines a confirmed
case of anthrax as 1) a clinically compatible case of cutaneous, inhalational, or
gastrointestinal illness that is laboratory confirmed by isolation of B. anthracis
from an affected tissue or site or 2) other laboratory evidence of B. anthracis
infection based on at least two supportive laboratory tests. CDC defines a suspect case as 1) a
clinically compatible case of illness without isolation of B. anthracis and no
alternative diagnosis, but with laboratory evidence of B. anthracis by one
supportive laboratory test or 2) a clinically compatible case of anthrax epidemiologically
linked to a confirmed environmental exposure, but without corroborative laboratory
evidence of B. anthracis infection.
“Consumer Alert “ regarding
antibiotics sold on-line
Consumers
who are visiting Web sites and receiving e-mail claiming to sell Ciprofloxacin (Cipro) and
other antibiotics to treat anthrax should consult a new “Consumer Alert” before
they buy products online, according to the Federal Trade Commission (FTC). The Alert,
"Offers to Treat Biological Threats: What You Need to Know," was produced by the
FTC, in conjunction with CDC and the Food and Drug Administration (FDA). The report is
available online at www.ftc.gov/opa/2001/11/alert.htm
Update: New York
anthrax investigations and WTC survey
The 61-year-old employee of Manhattan
Eye, Ear, and Throat Hospital (MEETH) who contracted inhalation anthrax, died as a result
of her illness. Thus far, all environmental samples from both MEETH, as well as the
individual's home, have tested negative for the presence of anthrax. At this point, the source of exposure to anthrax
remains under investigation. As part of an on-going comprehensive epidemiological
investigation, the New York City Department of Health, in collaboration with CDC, has
interviewed over 250 co-workers and close contacts in an effort to establish a source of
exposure. Further testing will be done at MEETH and in the individual's home. Results are
not expected until later this week.
As a precautionary measure the Health
Department, working with Lenox Hill Hospital, has made antibiotics available to over 1,100
individuals who work in, visited, or were treated at MEETH since October 11. Nasal swabs
have been limited to those individuals who worked in the immediate area of the deceased.
Of the 28 nasal swabs, none tested positive for anthrax.
The New York City Department of Health (DOH), in collaboration with CDC, is conducting
a voluntary survey of lower Manhattan residents who have been affected by the World Trade
Center disaster. DOH is administering this survey to address concerns and needs expressed
by area residents pertaining to their mental and physical health.
For more information see www.ci.nyc.ny.us/html/doh/html/new/new.html.
HHS/CDC staff deployment update (as of October 31, 2001)
Washington,
D.C.
- 27 EIS
Officers
- 18
Epidemiologists
- 15 Industrial
Hygienists
- 4 Laboratorians
- 4 Media Specialists
- 2 National Pharmaceutical Stockpile staff
- 4 Nurses
- 10 Public
Health Advisors
- 5 Public Health Prevention Specialists
- 1 Medical Officer
Trenton, N.J.
- 7 EIS Officers
- 5 Epidemiologists
- 1 Industrial Hygienist
- 1 Information Technology Specialist
- 1 Media Specialist
- 2 Public Health Advisors
New
York City (Anthrax)
- 21 EIS
Officers
- 8 Epidemiologists
- 4 Industrial Hygienists
- 4 Laboratorians
- 1 Media Specialist
- 5 Public Health Advisors
- 1 Public
Health Prevention Specialists
New York City (WTC)
- 3 EIS Officers
- 2 Industrial Hygienists
Phoenix, AZ
- 2 EIS Officers
- 1
Epidemiologist
West Palm Beach, FL
- 4 EIS
Officers
- 3
Epidemiologists
- 1 Industrial
Hygienist
- 1
Laboratorian
- 1 Media
Specialist
- 1 Medical
officer
- 1 Public
Health Advisor
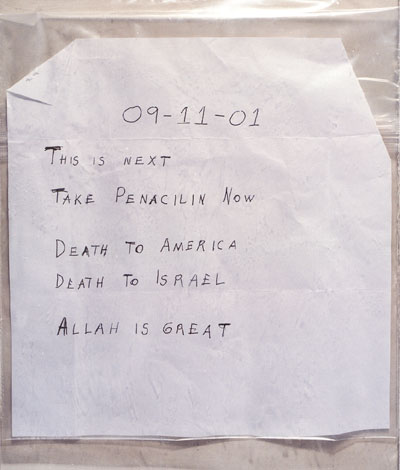
FDA PUBLIC HEALTH ADVISORY:
UPDATE ON USE OF DOXYCYCLINE FOR ANTHRAX EXPOSURE
Secretary of Health and Human Services Tommy G. Thompson announced on
October 17 in testimony before the Committee on Governmental Affairs and Subcommittee on
International Security, Proliferation and Federal Services of the United States Senate,
that the Food and Drug Administration is approving new labeling for the use of several
antibiotics to treat anthrax.
The following is being issued to provide healthcare providers with clarification on
dosing regimens about doxycycline. In addition, FDA is developing more information about
the use of this and other antibiotics to treat anthrax and will provide this information
soon.
Doxycycline is approved for the treatment of anthrax in all its forms. The FDA is
providing additional information concerning the dosing regimen for the treatment of
anthrax, including cutaneous and inhalation anthrax (post-exposure). The currently
recommended dosage regimen of doxycycline for severe disease is 100 mg every 12 hours for
adults and 1mg per pound (2.2mg per kilogram) every 12 hours for children less than 100
pounds. These dosage regimens are appropriate for use in patients who have been exposed to
anthrax (Bacillus anthracis) regardless of the route of exposure.
FDA and other health authorities strongly discourage individuals from taking any
antibiotic for prevention of anthrax without the specific advice of a physician and a
clear indication that exposure to the organism may have occurred.
- Marketer of Dietary Supplement Purporting to
Treat Liver Diseases Agrees to Settle FTC Charges:
Must
Have Adequate Scientific Evidence in the Future
Liverite Products, Inc., based in Tustin, California, its two principals, and two other
individuals agreed to settle Federal Trade Commission charges that they made numerous
unsubstantiated claims in Internet, radio, and print ads about the ability of
"Liverite" dietary supplement products to treat or prevent a wide range of liver
diseases or disorders, including cirrhosis and hepatitis. In an agreement to settle the
charges, Liverite Products, Inc. and its principals will be required to pay $60,000 in
redress, and all of the defendants will be prohibited from claiming that the Liverite
products or any food, drug or dietary supplement treats, cures or prevents any disease or
disorder, unless they have scientific evidence to support the claims.
The FTC's complaint names Liverite Products, Inc., Corinne and Steven Jacobson, and
James and Sheri Grant. According to the complaint, defendants Corinne and Steven Jacobson
direct and control Liverite Products, and defendants James and Sheri Grant developed the
websites through which the Liverite products were advertised and sold. The Liverite
products included: Liverite, the Ultimate Liver Aid; Liverite 3 in 1 for Men; Liverite 3
in 1 for Women; and Liverite Sports. The primary ingredient in each of these products was
extract of beef liver. The products were sold at retail outlets, such as GNC and CVS, by
telephone, and on the Internet at "liverite.com,"
"liveriteproducts.com," and "healthylifemarketing.com."
According to the FTC's complaint, the defendants' advertisements represented that
Liverite can prevent and treat hangovers; prevent and treat alcohol-induced liver disease,
including cirrhosis; treat liver diseases, including cirrhosis and hepatitis; and
alleviate the toxic side effects of various drugs. The FTC complaint alleges that these
representations were not supported by competent and reliable scientific evidence. The
complaint further alleges that the defendants falsely claimed that clinical tests proved
that Liverite is effective for the treatment of liver problems.
In addition to the defendants' advertisements that made unsubstantiated claims, the
defendants also used "metatag" technology to deceive consumers. Metatags are key
words embedded in the source code for a webpage that are invisible to the average
consumer, but are used by search engines to respond to consumers' search requests. The
complaint also alleges that the defendants embedded in the metatags of the Liverite
websites terms such as AIDS, hepatitis A, B & C, liver problems, liver disease, liver
detoxification, alcohol, hangover, cirrhosis, anabolic steroids, interferon, and
hepatatoxicity, thereby increasing the likelihood that consumers who researched these
topics on the Internet would be directed to defendants' websites.
The proposed stipulated final order, which requires the court's approval, will require
the defendants to have scientific substantiation that the Liverite products or any food,
drug, or dietary supplement:
- is effective in the prevention and treatment of hangovers and liver damage due to
alcohol consumption, cirrhosis or hepatitis;
-
- is effective in the treatment of cirrhosis, hepatitis, damaged liver, and candida
imbalance;
-
- is superior to traditional treatments for hepatitis C;
-
- lowers or regulates liver enzymes, restores liver cell integrity, and improves liver
function;
-
- prevents liver damage and other side effects from use of pain killers, allergy
medications, prescription drugs, interferon, medications used for Hepatitis C and HIV,
immuno-suppressant drugs, chemotherapeutic drugs, cholesterol-lowering drugs, and anabolic
steroids;
-
- protects and detoxifies the liver from toxins in the diet and environment; and
- reduces body fat.
The proposed stipulated final order also will require the defendants to possess
scientific substantiation for claims that any food, drug or dietary supplement can treat,
cure, alleviate the symptoms of, prevent, or reduce the risk of developing any disease or
disorder. In addition, the defendants cannot claim that any Liverite product is "the
ultimate liver aid," unless the claim is scientifically substantiated. The defendants
also will be prohibited from misrepresenting the results of any test or study, and will be
prohibited from misrepresenting that any testimonial or endorsement is the typical or
ordinary experience of users of the advertised product, unless the claim is substantiated.
Finally, the order requires Liverite Products, Inc. and the Jacobsons to pay $60,000.
The order would allow the defendants to make any claims that are approved for labeling
by the Food and Drug Administration. The order also includes various recordkeeping and
reporting requirements to help the FTC monitor the defendants' compliance with the order.
The Commission vote to authorize staff to file the complaint and proposed stipulated
final order was 5-0. They were filed in the U.S. District Court for the Central District
of California, Southern Division, in Santa Ana, on August 20, 2001, and require the
court's approval.
-
NEW JOINT PROGRAM ANNOUNCED BY FDA AND NCI HOLDS
PROMISE FOR CANCER
The Food and Drug Administration (FDA) and the National Cancer Institute (NCI)
announced today a new joint research and clinical program that holds great promise for
developing better and more targeted treatments for cancer. The new program, called the
Clinical Proteomics Program, melds the study of all proteins in living cells (or
proteomics) to the clinical care of patients, the first time this new research technology
has been applied directly to patient care.
"This new approach to treatment holds the potential to revolutionize cancer
detection and care," said Health and Human Services Secretary Tommy G. Thompson.
"With this expanded collaboration, the FDA and NCI are employing powerful, new
technologies they developed jointly." The agency collaboration began in 1997 and is
led by Emanuel Petricoin, Ph.D., of FDA's Center for Biologics Evaluation and Research
(CBER), and Lance Liotta, M.D. Ph.D., of NCI's Center for Cancer Research.
The new Clinical Proteomics Program, funded for three years with $1.1 million per year,
begins in the laboratory with recently developed tools capable of rapidly scanning cells
for hundreds of proteins at once. Petricoin and Liotta have also created new technologies
to generate protein fingerprints that may provide early warning of drug side effects. In
addition, they have already invented or refined several key technologies used in proteomic
analysis.
"The great challenge now in proteomics research is to begin to apply these
technologies to clinical care," said Petricoin. "We hope to take these
techniques out of the lab to assess their benefit for people with cancer, in a true
bench-to-bedside clinical research program."
"The potential payoffs for this program are great, said Liotta. "Everything
we learn while refining these cutting-edge technologies will benefit cancer patients and
the people trying to help them.
Potential benefits include:
- developing individualized therapies using targeted treatments that have been
predetermined to be effective for each patient;
- determining the toxic and beneficial effects of treatments first in the lab before using
them in patients;
- diagnosing cancer earlier than is now possible;
- improving the understanding of tumors at the protein level, leading to better
treatments.
Petricoin and Liotta have identified more than 130 proteins in cancers of the breast,
ovary, prostate, and esophagus that change in amount as the cells in these tissues grow
abnormally, which may provide new means of diagnosing and treating cancers earlier.
The first step to take these techniques out of the lab to benefit patients has begun
with the new FDA/NCI collaborative program. Through the Clinical Center at NIH, biopsied
cells from cancer patients before and after treatment are extracted using a special
microscope invented in Liotta's laboratory. The microscope allows them to isolate pure
normal cells, pre-cancerous cells, and tumor cells from the same patient. By capturing
cells directly from the tissue, the original protein pattern of the cells is maintained,
which is not the case with traditional methods of isolating cells.
Next, the scientists are analyzing the patterns of proteins in the extracted tumor
cells after the patient has been treated. For instance, the researchers are trying to
determine how a particular treatment changes the pattern of the proteins in a cell or
whether the protein patterns change if the tumor returns after treatment.
The NCI has recently begun clinical trials using proteomics to help make decisions
about the course of the patients' experimental treatments.
-
BAYER VOLUNTARILY WITHDRAWS
BAYCOL
FDA today announced that Bayer Pharmaceutical Division is voluntarily withdrawing
Baycol (cerivastatin) from the U.S. market because of reports of sometimes fatal
rhabdomyolysis, a severe muscle adverse reaction from this cholesterol-lowering
(lipid-lowering) product. The FDA agrees with and supports this decision.
Baycol (cerivastatin), which was initially approved in the U.S. in 1997, is a member of
a class of cholesterol lowering drugs that are commonly referred to as
"statins." Statins lower cholesterol levels by blocking a specific enzyme in the
body that is involved in the synthesis of cholesterol. While all statins have been
associated with very rare reports of rhabdomyolysis, cases of fatal rhabdomyolysis in
association with the use of Baycol have been reported significantly more frequently than
for other approved statins.
Fatal rhabdomyolysis reports with Baycol have been reported most frequently when used
at higher doses, when used in elderly patients, and particularly, when used in combination
with gemfibrozil (LOPID and generics), another lipid lowering drug. FDA has received
reports of 31 U.S. deaths due to severe rhabdomyolysis associated with use of Baycol, 12
of which involved concomitant gemfibrozil use.
Rhabdomyolysis is a condition that results in muscle cell breakdown and release of the
contents of muscle cells into the bloodstream. Symptoms of rhabdomyolysis include muscle
pain, weakness, tenderness, malaise, fever, dark urine, nausea, and vomiting. The pain may
involve specific groups of muscles or may be generalized throughout the body.
Most frequently the involved muscle groups are the calves and lower back; however, some
patients report no symptoms of muscle injury. In rare cases the muscle injury is so severe
that patients develop renal failure and other organ failure, which can be fatal.
Bayer Pharmaceutical Division has announced plans to withdraw Baycol to the pharmacy
level. Pharmacies will be instructed to return the product to the manufacturer for a
refund.
Patients who are taking Baycol should consult with their physicians about switching to
alternate medications to control their cholesterol levels. Patients taking Baycol who are
experiencing muscle pain or are also taking gemfibrozil should discontinue Baycol
immediately and consult their physician.
There are five other statins available in the U.S. that may be considered as
alternatives to Baycol. They are: lovastatin (Mevacor), pravastatin (Pravachol),
simvastatin (Zocor), fluvastatin (Lescol), and atorvastatin (Lipitor).
For further information regarding the withdrawal of Baycol, patients and physicians can
contact Bayer Customer Service 1-800-758-9794 or the FDA's Drug Information Office at
301-827-4573 or 1-888-INFO-FDA, or go to
"Baycol
Information" on FDA's Website.
-
FDA CLEARS CAMERA PILL TO PHOTOGRAPH SMALL
INTESTINE
FDA today cleared for marketing a swallowable capsule containing a tiny camera that
snaps pictures twice a second as it glides through the small intestine.
The product represents a technological advance in methods of examining the
gastrointestinal tract.
The device, made by Given Imaging Ltd., an Israeli company with North American
headquarters in Norcross, Ga., is intended to visualize the inside of the small intestine
to detect polyps, cancer, or causes of bleeding and anemia.
Currently the standard method of detecting abnormalities in the intestines is through
endoscopic examination in which doctors advance a scope down into the small intestine via
the mouth. However, these scopes are unable to reach through all of the 20-foot-long small
intestine, and thus provide only a partial view of that part of the bowel.
The camera capsule is designed to take photos of the entire small intestine, enabling
doctors to see areas that the endoscope cannot reach.
The device, called the Given Diagnostic Imaging System, comes in capsule form and contains
a camera, lights, transmitter and batteries. The capsule has a clear end that allows the
camera to view the lining of the small intestine.
The patient swallows the capsule, and the natural muscular waves of the digestive tract
propel it forward through the stomach, into the small intestine, through the large
intestine, and then out in the stool. The capsule transmits the images to a data recorder,
which is worn on a belt around the patient's waist. The physician then transfers the
stored data to a computer for processing and analysis.
The battery has an expected life of eight hours, which is generally long enough to
photograph the small intestine, but not long enough to photograph the entire
gastrointestinal tract.
FDA cleared the device based on both animal and clinical studies of safety and
effectiveness conducted by the manufacturer. In one of the human trials, Given Imaging
studied the use of the camera capsule in patients with suspected small intestine disease.
All patients had signs of either unexplained chronic gastrointestinal blood loss or
anemia. All had undergone standard endoscopic and radiological evaluations prior to
receiving the capsule.
Study results showed that the camera pill was safe, without any side effects, and was
able to detect abnormalities in the small intestine, including parts that cannot be
reached by the endoscope.
FDA cleared the device for use along with--not as a replacement for--other endoscopic
and radiological evaluations of the small bowel. The capsule was not studied in the large
intestine.
The product is available by prescription only.
-
Merrill Settles Suit Over Blodget's Stock Call
Merrill Lynch & Co. settled a high-profile arbitration case brought by a former client
who claimed he was misled by a bullish stock call by technology-stock analyst Henry
Blodget, potentially paving the way for similar actions by other aggrieved investors,
Friday's Wall Street Journal reported.
The nation's largest brokerage firm agreed to
pay $400,000 to Debases Kanjilal, a 46-year-old pediatrician, capping a case he filed in
March with the New York Stock Exchange, according to people with knowledge of the matter.
In the civil case, Mr. Kanjilal contended that Mr. Blodget maintained a "buy"
recommendation on InfoSpace Inc., an Internet stock, to support a lucrative financial deal
for Merrill. Mr. Kanjilal said he had a loss of about $500,000, following Mr. Blodget's
advice.
The case could have broader ramifications for the brokerage business, which has come
under pressure in recent months for conflicts involving often-bullish research it provides
to investors.
Arbitration cases have no precedential value, of course, and investors would have had
to have suffered big losses to make it worthwhile for them to pursue similar claims
against Wall Street firms or analysts.
Still, by settling the matter, Merrill (MER) could open the door for more legal action
by investors who believe they were burned by snapping up shares of once-highflying
technology stocks hyped by, among other things, aggressive buy recommendations by
analysts. In most cases, Wall Street firms only made minimal disclosures about any
potential conflicts, including lucrative investment-banking relationships with firms whose
stocks they were touting.
-
Foreign and Domestic Investors-Merrill
Lynch: A Bunch Of Bull-Abandons the small investor leaving them victims to fraud-PART II
Within 24 hours of this expose', the guilty
credit card scheme is revealed, and confession by a "nineteen year old" Internet
executive is made absent any work or help from Merrill Lynch; inconsistent though
demonstrative of the positive influence of this press. More soon on this Merrill
Lynch investor case; InfoJustice.
Foreign and Domestic Investors-Merrill
Lynch: A Bunch Of Bull-Abandons the small investor leaving them victims to fraud!
An investor advised that they had a small account
approximately $15,000. They received their statement on this past Friday and noted
they were down $2,000. and their were fraudulent charges on a Merrill Lynch Visa.
When the investor called on Monday morning, they were informed that Merrill Lynch made a
International decision to send all class one investors to a team of specialists which is
better than a broker. When the investor explained they only went to Merrill Lynch
for the benefit of a local neighborhood broker and not a team in New Jersey (the investor
account was in Los Angeles) he was told in essence "tough bounce" (Well there
goes the investors Roth Ira?). The Torrance branch refused to discuss the fact that
a fraud had been found and would not help. They then claimed this was on the most
recent statement. The investor revealed the fraud was on the most recent statement
and that there was no mention of Merrill Lynch abandoning investors. Well, our
investor caught this slight of hand tactic, and it will be next month allegedly that the
"Big Bull" will inform investors. Yet Merrill Lynch refused to help our
investor catch the fraud prior to his notification of any Merrill Lynch Corporate changes
to this families hard earned monies.
Our investor then called
the corporate offices of Merrill Lynch in New York only to find one cannot complain to the
President as "he has no phone"!. In fact they have no mechanism or
internal affairs to investigate mismanagement or internal fraud! After many more
calls he was forwarded to Merrill Lynches attorney and their Credit Card Fraud
investigators (fine retired New York PD detectives). Finally our investor found the
facts. The Detective explained that our investor contact the fraudulent credit card
office (which they did and file a complaint) and cancel the card. Then the complaint
comes to him! They further had to send a letter to the "Big Bully-Lynch"
about the fraudulent charge (which they did). Further the retired detective advised
that this had just happened to him, but he lives in New Jersey and does not mind the local
call. He further advised that Merrill Lynch is in my language, dumping anyone they
considered a small investor to this non-preferred system of dealing with computers, long
lines of callers ahead of you to purchase/sell funds, report missing money and answer
machines in lieu of a Broker.
Thus only through our
investors own vigilance will the credit card fraud or error (which ever) be eliminated and
their money returned. The Torrance branch manager refused to take our civilian
investors calls or return the call as it would not make big dollars for the bull;
obviously. Yet my question's remain. Were
is the investors missing money, and to what end will they
have to go to have their entire account reviewed with the "governing bodies" and
establish corporate abandonment of services and a form of "internal/corporate
fraud"? Lets face it this is a clear case where the
investor sought out a Broker account and was bait and switched into a "team of
experts" manned by answer phones, long lines on the telephone (you are caller number
109 please hold on to discuss your Merrill Lynch Loses) and failure to have any control or
policing of investments. The investor advises numerous failures such as inability to
get requested deposit slips with I.D. and account number on them for one year, and
numerous occasions where similar funds in others accounts failed to post similar loses,
and deposited moneys earmarked for select stock purchases were not made and moneys went to
margins.
International investors, beware, if you have a problem in your country you
will never get any action if you have a problem and invest in Merrill Lynch.
Domestic investors watch your money like a hawk and get the heck out of Merrill Lynch or
you to may get caught up in a bunch of Bull. It amazes this examiner what companies
will do when earnings are down: (Editor's note.
The following day after this article was posted, Merrill Lynch announced lower
earnings expected in august-MOTIVE to lower internal costs such as broker volume at the
expense of investors. Transactions down 41%, and believes third quarter worse.
Standard @ drops Merrill Lynch ratting to "Poor" noting a cost side cut
into profits; cutting cost by laying off the work force through select staff reduction no
matter how it affects its investors. So much for
the Merrill Lynch mission to advise investors to their best interests;inconsistent ) InfoJustice
FTC Announces a Second Case Focusing on
Safety Risks of Comfrey Products Promoted via Internet
The Federal Trade Commission today is announcing a second case challenging the
marketing and selling of unproven and dangerous comfrey products via the Web, as part of
its ongoing and comprehensive "Operation Cure.All" initiative. The target of
today's action is Western Botanicals, Inc., a Fair Oaks, California company that
manufactured and marketed a variety of products containing the herbal ingredient comfrey,
for both external and internal uses. The FTC charges that the company made unfounded
claims that the products were beneficial in the treatment of a wide variety of serious
diseases and health conditions, and that they were safe. In fact, comfrey contains toxic
substances and, when taken internally, can lead to serious liver damage, according to the
FTC. Western Botanicals has agreed, in a stipulated permanent injunction filed in federal
court, to stop marketing comfrey products for internal uses or on open wounds, and to
include a warning on comfrey products marketed for external uses. It has also agreed to
stop making the challenged safety and health benefit claims.
"The Internet is a powerful tool for consumers searching for health
information," said Howard Beales, Director of the FTC's Bureau of Consumer
Protection. "Unfortunately, it's also an outlet for unscrupulous marketers who use
deceptive promotions to peddle their products. Consumers who delay or forego treatment
while using unproven products that promise miracles can increase their health risks
unnecessarily."
According to the FTC, Western Botanicals, its president, Randy C. Giboney, and
vice-president, Kyle D. Christensen, marketed and sold herbal products containing comfrey
to distributors and directly to consumers by mail, newsletters, and on the Internet at www.westernbotanicals.com.
The products purportedly treated and alleviated symptoms of various diseases and health
conditions. In their advertising and promotional materials the defendants represented
their comfrey products were safe for consumers, including nursing women, when taken
internally or applied to open wounds. The defendants also claimed that their comfrey
products, when taken internally, would treat chronic bronchial diseases, gastritis,
duodenal ulcers, colitis, rheumatism, arthritis, osteoporosis, multiple sclerosis,
amyotrophic lateral sclerosis and other conditions. The FTC alleges that the defendants'
representation that their comfrey products were safe is false, and that they did not have
scientific evidence to substantiate their safety or efficacy claims.
The defendants have agreed to a stipulated final order for permanent injunction to
resolve the FTC allegations. The stipulated final order would prohibit them from marketing
any comfrey product for ingestion, for use as a suppository, or for external use on open
wounds, unless they have evidence that the product is free of pyrrolizidine alkaloids and
is safe. They would also be required to place the following disclosure warning in any
advertisement, promotional material or product label for any comfrey products intended for
topical use:
WARNING: External Use Only. Consuming this product can cause serious
liver damage. This product contains comfrey. Comfrey contains pyrrolizidine alkaloids,
which may cause serious illness or death. This product should not be taken orally, used as
a suppository, or applied to broken skin. For further information contact the Food and
Drug Administration: http//vm.cfsan.fda.gov
In addition, the order would prohibit the defendants from making the specific health
claims challenged in the complaint or any unsubstantiated representations about the
safety, health benefits, performance, or efficacy of any food, drug, dietary supplement or
other health-related product or service. The order further would require them to notify
their distributors that unsubstantiated claims violate the law and that the defendants
will terminate distributors who make false or unsubstantiated claims. The stipulated order
includes a suspended judgment of $50,800 and a right to reopen provision that would
reinstate the judgment if the court finds that the defendants made material
misrepresentations or omissions on their financial statements. Finally, the order includes
various recordkeeping and reporting requirements designed to assist the FTC in monitoring
the defendants' compliance.
On Friday July 6, 2001, the Food and Drug Administration issued a letter to industry
communicating concern about the safety of supplement products containing comfrey. FDA's
letter, which has been sent to trade associations and other industry groups, advises that,
because comfrey contains certain toxic substances - pyrrolizidine alkaloids - that have
been associated with liver damage and other health hazards, it should not be used as an
ingredient in supplements. FDA further recommends that firms immediately stop marketing
comfrey-containing supplements and alert consumers to stop using the products. Finally,
FDA is urging manufacturers to identify and report any adverse events, including liver
disorders, that have been associated with comfrey and other ingredients containing
pyrrolizidine alkaloids. The letter is also posted on FDA's website at www.cfsan.fda.gov
The Food and Drug Administration has been a close partner of the FTC and assisted the
agency in today's enforcement action, as well as many other aspects of "Operation
Cure.All." The FTC also thanks the Texas Department of Health for its participation
in this phase of "Operation Cure.All."
The Commission vote authorizing staff to file the complaint and proposed stipulated
judgment in the Western Botanicals case was 5-0. They were filed in the U.S. District
Court, Eastern District of California, in Sacramento, on July 11, 2001. The proposed
judgment is subject to court approval.
CDC WARNS ABOUT EXTREME
HEAT
Each year more people in the United States die from extreme heat than
from hurricanes, lightning, tornadoes, floods, and earthquakes combined. During 1979-1998, a total of 7,421 deaths that
occurred in this country were attributed to excessive heat exposure. On average
approximately 300 people die each year from exposure to heat. This year extreme heat is of particular concern
because of the energy problems facing many areas of the country. Air conditioning is the number-one protective
factor against heat-related illness and death. Brownouts
that last a few hours will likely have little effect on people’s health. However, some people may be fearful of high utility
bills and limit their use of air conditioning. Such action can place people who are
already at risk for heat illness at increased risk. You can help by learning the warning
signs of heat stroke and heat exhaustion and then checking on your neighbors frequently.
FDA Issues Guidance on Levothyroxine Sodium
Products Compliance
The Food and Drug Administration today published a guidance for industry explaining how
the agency plans to handle oral levothyroxine sodium products that are being marketed
without an approved application after August 14, 2001.
On August 14, 1997, FDA announced in the Federal Register (62 FR 43535) that
orally administered levothyroxine sodium drug products are "new drugs" and that
manufacturers who wish to continue marketing these products must submit a new drug
application (NDA) for approval. The agency based its decision on a history of potency and
stability problems with orally administered levothyroxine sodium products. The notice
stated that after August 14, 2000, any unapproved levothyroxine sodium drug product on the
market would be subject to regulatory action by FDA.
On April 26, 2000, FDA extended the deadline to August 14, 2001. As of July 2001, two
levothyroxine sodium products have been approved by FDA to treat hypothyroidism.
Unithroid, manufactured by Jerome Stevens Pharmaceuticals, was approved on August 21,
2000. Levoxyl, manufactured by Jones Pharma, was approved on May 25, 2001. Now that two
products have been approved, FDA is issuing guidance regarding the transition of patients
from unapproved to approved products.
Because there is no public health emergency that requires an immediate switch to the
approved drugs, FDA has established a gradual phase out of distribution of the unapproved
products to allow manufacturers of approved products to scale up to meet demand and to
allow adequate time for patients and health care providers to make an orderly transition
from unapproved to approved products.
On August 14, 2001, there will be two types of unapproved marketed levothyroxine sodium
products: (1) those with NDAs that have been submitted to FDA and are under review and (2)
those with no pending NDAs.
Under the phase out outlined in the guidance, manufacturers of unapproved oral
levothyroxine sodium drug products with NDAs pending as of August 14, 2001, should reduce
the distribution of these products according to an incremental reduction of average
monthly distribution. This phase-out schedule is explained in the guidance. By August 14,
2003, all distribution of unapproved oral levothyroxine sodium products must cease.
Manufacturers of unapproved oral levothyroxine sodium drug products who do not have an
NDA pending with the FDA by August 14, 2001, should cease distribution of their products
by that date or they will be subject to regulatory action.
The FDA is warning consumers to discontinue use of thirteen Chinese herbal
products containing aristolochic acid because they may present a serious health hazard to
consumers. Aristolochic acid found in certain plants and botanicals is toxic to the
kidneys and is a potent carcinogen. This chemical can cause serious kidney damage and the
use of products that contain aristolochic acid has been associated with several
occurrences of kidney failure. The use of aristolochic acid-containing products has also
been linked to increased risk of kidney cancer in people who have consumed it.
Blue Light, Inc., Ithaca, N.Y., has initiated a recall of these products
sold under the "Treasure of the East" label with "MFG No.
200008" (2000=year, 08=month) and earlier production dates. Products with "MFG
No. 200009" and later production dates are not affected.
Products include:
| Item # |
Single-ingredient |
| 100176-0 |
Guan) Mu Tong |
| 100644-2 |
Ma Dou Ling (Mi) |
| Item # |
Herbal combinations |
| B015 |
Ba Zheng San |
| D060 |
Dang Gui Si Ni Tang |
| D075 |
Dao Chi San |
| F050 |
Fu Fang Di Hu Tang |
| G005 |
Gan Lu Xiao Du Dan |
| K030 |
Kou Yan Ning |
| L070 |
Long Dan Xie Gan Tang |
| P005 |
Pai Shi Tang |
| X072 |
Xiao Ji Yin Zi |
| X125 |
Xin Yi San |
| Y020 |
Yang Yin Xiao Yan Tang |
These products were distributed nationwide in small quantities primarily
to acupuncturists, herbalists, and herbal stores. They are in powder form (3.5 oz.
bottles) or capsule form (100 per bottle) under the "Treasure of the East"
label.
The recall was initiated as a result of public health concerns associated
with the consumption of aristolochic acid products. No illnesses have been reported. Blue
Light, Inc., has discontinued the distribution and use of products that may contain
aristolochic acid.
Consumers who have purchased any of these products with affected
expiration dates should discontinue their use and may return them to place of purchase for
a full refund. Consumers with questions may contact the company at 1-888-258-3548.
FDA APPROVES TWO NEW INTRAOCULAR
PRESSURE LOWERING DRUGS FOR THE MANAGEMENT OF GLAUCOMA
The Food and Drug Administration (FDA) announced the approval of two new
drugs to treat the elevated intraocular pressure which is often associated with glaucoma -
Lumigan (bimatoprost ophthalmic solution) 0.03% and Travatan (travoprost ophthalmic
solution) 0.004%. They will provide additional alternatives for the reduction of
intraocular pressure in patients who are intolerant of other intraoular lowering
medications, or in patients who have had insufficient responses to other intraocular
pressure lowering medications. Many of these patients might otherwise need surgery for
management of their glaucoma.
Glaucoma, a leading cause of irreversible blindness in the world, is the
second most common cause of blindness in the United States. Glaucoma represents a family
of diseases commonly associated with optic nerve damage and visual field changes (a
narrowing of the eyes’ usual scope of vision). Elevated intraocular pressure is a
primary risk factor for glaucoma.
"Glaucoma is a serious eye disease affecting some two million older
Americans," said Health and Human Services Secretary Tommy G. Thompson. "Early
detection of glaucoma and management of raised eye pressure can usually prevent vision
loss. These new drugs provide additional treatment alternatives to preserve vision as well
as preserve an individual’s quality of life."
In separate clinical trials, Lumigan and Travatan had similar effects in
lowering intraocular pressure. Higher intraocular pressures greatly increase the risk of
optic nerve damage and vision loss.
Side effects associated with Lumigan and Travatan may include gradual
darkening of eye color, darkening of eyelid skin, and increased thickness, number, and
darkness of eyelashes.
The availability of multiple medical alternatives provides physicians with
additional treatment options for their patients whose glaucoma is difficult-to-manage.
Lumigan will be marketed by Allergan, Inc. of Irvine, California. Travatan
will be marketed by Alcon Universal, Ltd of Fort Worth, Texas.
NEWLY FORMULATED DTaP (DIPHTHERIA, TETANUS, AND
PERTUSSIS) VACCINE APPROVED WITH ONLY TRACE AMOUNTS OF THIMEROSAL
Today, the FDA approved a newly formulated version of Tripedia, a diphtheria and
tetanus toxoids and acellular pertussis (DTaP) vaccine without preservatives and with only
a trace amount of thimerosal.
"This approval is significant because now all routinely recommended pediatric
vaccines will be available as either completely thimerosal free or without any significant
amounts of thimerosal, a preservative that contains mercury," said Dr. Bernard
Schwetz, Acting Principal Deputy Commissioner. "Although thimerosal is a very
effective preservative, the Public Health Service recommended that thimerosal should be
reduced or eliminated from vaccines as soon as possible to minimize the exposure of
infants and young children to mercury."
Tripedia now contains less than 0.5 micrograms of mercury per dose, a greater than 95%
reduction in the amount of thimerosal per dose compared to the original version of
Tripedia.
The pediatric vaccines that are recommended for routine use are: DTaP, hepatitis B,
Haemophilus conjugate (Hib), pneumococcal conjugate, inactivated poliovirus, varicella,
measles, mumps and rubella. Since 1999, pediatric formulations of hepatitis B vaccines
that either contain no thimerosal (Recombivax HB) or trace amounts (EngerixB) have been
approved.
In recent years, various federal agencies have been addressing the health risks of
mercury, which is found in the environment, in food and in household products. Although no
harmful effects have been reported from thimerosal at doses that were used in vaccines,
the PHS agencies, the American Academy of Pediatrics, and vaccine manufacturers agreed
that thimerosal should be reduced or eliminated in vaccines to make already safe vaccines
even safer.
FBI ARRESTS AGENT FOR ESPIONAGE
Attorney General John Ashcroft, FBI Director Louis J. Freeh
and United States Attorney Helen Fahey announced today that a veteran FBI
counterintelligence Agent was arrested Sunday by the FBI and charged with committing
espionage by providing highly classified national security information to Russia and the
former Soviet Union.
At the time of the arrest at a park in Vienna, Virginia,
Robert Philip Hanssen, age 56, was clandestinely placing a package containing highly
classified information at a pre-arranged, or "dead drop," site for pick-up by
his Russian handlers. Hanssen had previously received substantial sums of money from the
Russians for the information he disclosed to them.
FBI Director Louis J. Freeh expressed both outrage and
sadness. He said the charges, if proven, represent "the most serious violations of
law -- and threat to national security."
"A betrayal of trust by an FBI Agent, who is not only
sworn to enforce the law but specifically to help protect our nation's security, is
particularly abhorrent. This kind of criminal conduct represents the most traitorous
action imaginable against a country governed by the Rule of Law. It also strikes at the
heart of everything the FBI represents -- the commitment of over 28,000 honest and
dedicated men and women in the FBI who work diligently to earn the trust and confidence of
the American people every day."
"These kinds of cases are the most difficult,
sensitive and sophisticated imaginable. I am immensely proud of the men and women of the
FBI who conducted this investigation. Their actions represent counterintelligence at its
very best, reflecting dedication to both principle and mission. It is not an easy
assignment to investigate a colleague, but they did so unhesitatingly, quietly and
securely."
Hanssen was charged in a criminal complaint filed in
Federal court in Alexandria, Virginia, with espionage and conspiracy to commit espionage,
violations that carry a possible punishment of life in prison, and under certain
circumstances, the death penalty. Following the arrest, FBI Agents began searching
Hanssen's residence, automobiles and workspace for additional evidence.
A detailed affidavit, filed in support of the criminal
complaint and search warrants, provides a troubling account of how Hanssen first
volunteered to furnish highly sensitive documents to KGB intelligence officers assigned to
the Soviet embassy in Washington, D.C. The affidavit chronicles the systematic transfer of
highly classified national security and counterintelligence information by Hanssen in
exchange for diamonds and cash worth more than $600,000. Hanssen's activities also have
links to other, earlier espionage and national security investigations including the
Aldrich Ames and Felix Bloch cases, according to the affidavit.
The affidavit alleges that on over 20 separate occasions,
Hanssen clandestinely left packages for the KGB, and its successor agency, the SVR, at
dead drop sites in the Washington area. He also provided over two dozen computer diskettes
containing additional disclosures of information. Overall, Hanssen gave the KGB/SVR more
than 6,000 pages of valuable documentary material, according to the affidavit.
The affidavit alleges that Hanssen compromised numerous
human sources of the U.S. Intelligence Community, dozens of classified U.S. Government
documents, including "Top Secret" and "codeword" documents, and
technical operations of extraordinary importance and value. It also alleges that Hanssen
compromised FBI counterintelligence investigative techniques, sources, methods and
operations, and disclosed to the KGB the FBI's secret investigation of Felix Bloch, a
foreign service officer, for espionage.
Freeh said that although no formal damage assessment could
be conducted before the arrest without jeopardizing the investigation, it is believed that
the damage will be exceptionally grave.
During the time of his alleged illegal activities, Hanssen
was assigned to New York and Washington, D.C., where he held key counterintelligence
positions. As a result of his assignments, Hanssen had direct and legitimate access to
voluminous information about sensitive programs and operations. As the complaint alleges,
Hanssen effectively used his training, expertise and experience as a counterintelligence
Agent to avoid detection, to include keeping his identity and place of employment from his
Russian handlers and avoiding all the customary "tradecraft" and travel usually
associated with espionage. The turning point in this investigation came when the FBI was
able to secure original Russian documentation of an American spy who appeared to the FBI
to be Hanssen, which subsequent investigation confirmed.
Freeh said the investigation that led to the charges is a
direct result of the combined and continuing FBI/CIA effort ongoing for many years to
identify additional foreign penetrations of the U.S. intelligence community. The
investigation of Hanssen was conducted by the FBI with direct assistance from the CIA,
Department of State and the Justice Department, and represents an aggressive and creative
effort which led to this counterintelligence success. Freeh said, "We appreciate the
unhesitating leadership and support of Attorney General John Ashcroft from the moment he
took office."
Freeh also expressed his gratitude to Helen Fahey, United
States Attorney for the Eastern District of Virginia, Assistant United States Attorney
Randy Bellows, and senior Justice Department officials Robert Mueller, Frances Fragos
Townsend, John Dion and Laura Ingersoll for their contributions to the case.
United States Attorney Fahey said, "In the past
decade, it has been our unfortunate duty to prosecute a number of espionage cases -- Ames,
Pitts, Nicholson, Squillacote, Kim, Boone, and others. With each case, we hope it will be
the last. Today, however with the arrest of Robert Hanssen, we begin again the process of
bringing to justice a U.S. Government official charged with the most egregious violations
of the public trust. The full resources of the Department of Justice will be devoted to
ensuring that those persons who would betray their country and the people of the United
States are prosecuted and severely punished."
"I want to express my appreciation for the outstanding
work done by the National Security Division and the Washington Field Office of the FBI in
this investigation. Their superlative work in this extraordinarily sensitive and important
investigation is testament to their professionalism and dedication. We also express our
deep appreciation for the outstanding assistance provided by the Internal Security Section
of the Criminal Division of the Department of Justice."
Freeh and CIA Director George Tenet kept the Intelligence
Committees of Congress, because of the clear national security and foreign policy
implications, informed about the case.
As a result of Hanssen's actions, Freeh has ordered a
comprehensive review of information and personnel security programs in the FBI. Former FBI
Director and Director of Central Intelligence William H. Webster will lead the review.
Webster, currently in private law practice, brings a "unique experience and
background in government management and counterintelligence," Freeh said.
"Moreover, the respect he enjoys throughout the intelligence community and elsewhere
in government is second to none. Judge Webster will have complete access and whatever
resources that are necessary to complete the task and will report directly to Attorney
General Ashcroft and me. I will share his report with the National Security Council and
then Congress as well," Freeh said .
SUDDEN CARDIAC DEATHS ARE INCREASING IN YOUNG
PEOPLE, ESPECIALLY AMOUNG YOUNG WOMEN
San Antonio — Yearly death totals of sudden cardiac death (SCD) in people between
the ages of 15 and 34 rose 10% overall during the past decade — from 2,719 in 1989 to
3,000 in 1996, according to data presented by researchers from the Centers for Disease
Control and Prevention (CDC) during the American Heart Association’s 41st Annual
Conference on Cardiovascular Disease Epidemiology and Prevention, in San Antonio, Texas.
Alarmingly, although the numbers are very small, the SCD death rate increased by 30% in
young women. Death rates were also higher among young African-Americans than whites.
"We can’t fully explain this increase in SCD among young people, particularly
young women," said CDC Director Jeffrey Koplan, M.D., M.P.H. "However, smoking
cigarettes, obesity, and lack of physical activity are high among adolescents. Poor
recognition of heart events in younger patients and delayed application of cardiopulmonary
resuscitation or defibrillation may also be contributing to this increase."
SCD typically is caused by ischemic heart disease, which restricts blood flow to the
heart; arrhythmia (irregular heart beat); or cardiomyopathy (deterioration of the heart
muscle). Ischemic heart disease has been associated with not being physically active,
eating a poor diet, and smoking cigarettes. Arrhythmia and cardiomyopathy are often
inherited or result from a structural problem in the heart.
Lifestyle changes, plus early identification of risk and prompt attention when signs of
heart distress are recognized, could help reduce SCD in people ages 15-34, according to
the CDC.
"Adopting a heart-healthy lifestyle that includes 30 minutes of moderate physical
activity on most days of the week, a low-fat diet with lots of fruits and vegetables, and
either stopping smoking or not starting, are three steps we all can take to help reduce
the risk of sudden cardiac death," said George A. Mensah, M.D., chief of
cardiovascular health at CDC and co-author of the report. "Families with a history of
early heart disease or sudden cardiac death should talk to their doctors about screening
younger family members."
The report was presented in San Antonio by lead author Zhi-Jie Zheng, M.D., Ph.D.,
epidemiologist. Other researchers included Janet Croft, Ph.D., and Wayne L. Giles, M.D.
CDC protects people’s health and safety by preventing and controlling diseases and
injuries; enhances health decisions by providing credible information on critical health
issues; and promotes healthy living through strong partnerships with local, national, and
international organizations.
- FDA UPDATES SAFETY INFORMATION FOR MICONAZOLE
VAGINAL CREAM AND SUPPOSITORIES
FDA is advising women who take the
prescription blood-thinner warfarin to consult their doctor or pharmacist for advice
before using an OTC vaginal miconazole product.
FDA has also advised manufacturers of vaginal creams and suppositories containing
miconazole to add a new warning to the Drugs Facts box on product labels. The warning
states: Ask a doctor or pharmacist before use if you are taking the prescription blood
thinning medicine warfarin, because bleeding or bruising may occur.
FDA is taking this action because the agency has received two adverse events indicating
abnormal blood clotting tests with women who took anticoagulant therapy and used vaginal
miconazole. In addition to abnormal tests, one woman developed bruises, bleeding gums and
a nosebleed. Two articles from medical journals reported cases of probable warfarin
interaction with vaginal miconazole. The agency believes that consumers should have all
the information about a drug’s potential risks before deciding to use it.
Miconazole is an antifungal drug that has been available by prescription and
over-the-counter in different forms such as creams and suppositories for many years. The
vaginal creams and suppositories are used to treat vaginal yeast infections.
The interaction of systemically administered miconazole with warfarin is well
established, and is included in the warfarin labeling. Because of the concerns raised by
the recent reports of an interaction with vaginally administered miconazole with warfarin,
physicians and patients should be aware that patients who need to use both products
simultaneously should be appropriately monitored. In addition to being placed on the
product labels, the new label will be included in consumer brochures. Products containing
miconazole include the recently approved Monistat combination pack.
FDA ISSUES HEALTH WARNING ABOUT AVOCADO
PULP IN SOUTHERN CALIFORNIA BECAUSE OF POSSIBLE HEALTH RISK
FDA is warning consumers in southern California not to consume avocado
pulp products from two distributors, G Products and T & G Sales, because these
products have the potential to be contaminated with Listeria monocytogenes, an
organism that can cause serious and sometimes fatal infections in young children, frail or
elderly people, and others with weakened immune systems. Although healthy individuals may
suffer only short-term symptoms such as high fever, severe headache, stiffness, nausea,
abdominal pain and diarrhea, Listeria infection can cause miscarriages and
stillbirths among pregnant women.
G Products is recalling three lots of its avocado products. T & G Sales was issued
a warning letter by the FDA on February 1, 2001.
The G Products bulk avocado pulp product was distributed in Southern
California, primarily to small Mexican style fast food restaurants in Orange, Riverside,
Los Angeles, and San Diego counties. T & G Sales bulk avocado pulp product was
distributed in San Diego County, primarily to small Mexican style fast food restaurants
from November 2000 through January 2001. These products, if frozen, have a shelf life of 3
to 4 months.
The G Products avocado pulp is packaged in bulk heat sealed, 6 pound, clear plastic
bags. Product labeling identifies the product as G Products Brand 100% Haas Avocado
"Pulp" or "Chunky" style. The date codes are stamped on the label as
"DEC 05 2000," "JAN 17 2001," and "JAN 30 2001."
The T & G Sales bulk avocado product is packaged in bulk heat sealed, 6 pound clear
plastic bags and 25 pound plastic pails.
No illnesses have been reported to date.
This recall is the result of routine sampling by the FDA at the time of importation.
FDA laboratory findings confirmed Listeria monocytogenes in lots from each
importer, and the importer was instructed to hold the lots intact and not distribute them.
However, these products were distributed without an FDA release.
It is recommended that restaurants that may have purchased avocado pulp products from
these companies check their inventories and discontinue using any of these products listed
above. Restaurant owners and concerned consumers with questions may call G Products at
619-295-7910 and T & G Sales at 619-232-9020 or 619-778-4957.
CDC AND WORLD BANK SIGN AGREEMENT TO IMPROVE
HEALTH IN DEVELOPING COUNTRIES
The Centers for Disease Control and Prevention (CDC) and the World Bank signed a
groundbreaking agreement today to work more closely together to improve health in
developing and transition countries through better communication, coordination, and
collaboration.
Under this agreement, CDC is assigning technical experts to the World Bank to
collaborate in the design, implementation, and evaluation of projects on prevention and
control of malaria in Africa; on environmental health in South Asia; on chronic diseases
such as cardiovascular disease and cancer, and their risk factors including tobacco abuse
in Latin America and in Eastern Europe/Central Asia; and on immunizations and vaccine
preventable diseases globally.
Dr. Jeffrey P. Koplan, CDC director, states, "The combination of CDC's health
knowledge, skills and experience, and the World Bank's economic know-how and development
capability make a powerful partnership to improve global health."
The broader range of global health activities will also include: nutrition, maternal
and child health, infectious diseases (e.g. HIV/AIDS, tuberculosis), public health, health
surveillance, health policy, program planning and evaluation, health statistics, health
economics, operational/applied research, health policy research, health services research,
and health care technology.
"To meet the development challenges of the 21st century, the World Bank needs to
strengthen its partnerships with other agencies to advance international understanding and
initiatives related to health, nutrition, and populations. We welcome this new opportunity
to extend our collaborative and cooperative efforts with the CDC," said Christopher
Lovelace, Director of the Health, Nutrition, and Population Sector at the World Bank.
The urgency is evident in the fact that, as Dr. Stephen Blount, Associate Director for
Global Health at CDC indicates, "Nearly 1.3 billion people, representing one fourth
of the world's population, continue to live in absolute poverty. Ninety-three percent of
the global disease burden is concentrated in low- and middle-income countries."
Most developing and transition countries face difficult challenges caused by continued
poverty, malnutrition, poor health, poor performance of many health systems, and
inadequate and/or unsustainable health care financing. The World Bank is the leading
global financial lender to low- and middle-income countries for development. The CDC is
recognized as a leader in global disease prevention and control. The World Bank/CDC
agreement was developed based on a recognition that a strong public-private partnership
between these two unique organizations was needed to better combat the threats to global
health.
The Centers for Disease Control and Prevention (CDC) protects people's health and
safety by preventing and controlling diseases and injuries; enhances health decisions by
providing credible information on critical health issues; and promotes healthy living
through strong partnerships with local, national and international organizations.
2001 FDA SCIENCE FORUM: SCIENCE ACROSS THE
BOUNDARIES
"Science Across the Boundaries" will be the theme for the 2001
FDA Science Forum to be held February 15-16 at the Washington Convention Center in
Washington, D.C. The forum will highlight issues in science that cross the boundaries of
industry, academia, government agencies, consumer groups and international constituents.
The forum will be sponsored by the FDA, AOAC International, formerly the
Association of Official Analytical Chemists, and Sigma Xi, a scientific research society.
The forum will address emerging issues connected to FDA's approach to new
technology such as privacy and confidentiality; modeling and simulation; leveraging and
partnerships across FDA boundaries, and laboratory accreditation.
On February 15, AOAC International will sponsor a mock laboratory
accreditation session.
On February 16, a "Breakfast with the Authors" session will be
held to allow individuals the opportunity to network and talk with the authors of
scientific posters representing all areas of FDA regulatory science.
As part of the second day's activities, the FDA Scientific Achievements
Awards of Excellence will be announced. In addition, an FDA Center Director Roundtable
session will be moderated by FDA's Office of Science Coordination and Communication.
For more information on the 2001 FDA Science Forum, please contact FDA's
Office of Science Coordination and Communication at 301-827-3340 or visit AOAC's website
for registration information at www.aoac.org.
LETTERS TO THE EDITOR:
Dear Dr. Neff. I was given your name by the
Blank...Minister...Blank. He advised you could steer me to actual scientific and
forensic contributions to the advancement of science and medicine. I must state that
as a chiropractic student in Australia, I find that we are locked out of the rest of the
medical system and am deeply discouraged about some of the irrational claims made by my
new colleagues.... Dear Jeff (I apologize for the
delay). I have only typed your opening statements as I feel that as you grow, you
will change your opinions and understand your colleagues through the wisdom of science and
practical clinical science. Don't be so hard on yourself. Your just beginning your
wonderful journey into the health care amalgam. Enclosed please find the following
link to my first published work, which changed the basis of physiology text books of the
day, as well as bringing DC's into their just realm of treating real conditions,
experienced by people today, rendering a real diagnosis, and offering the correct
consistent care. Your wonderful and adventurous journey into Chiropractic Forensic Science
begins here.
FDA ISSUES URGENT NOTICE OF RECALLED INJECTABLE
DRUGS
The Food and Drug Administration (FDA) is urging individuals, health care organizations
and medical product distributors to stop dispensing and/or distributing certain injectable
medications marketed by Phyne Pharmaceuticals of Scottsdale, Ariz. AMRAM Inc. of Rathdrum,
Idaho manufactured these products for Phyne Pharmaceuticals, who was their sole customer.
On December 14, 2000, AMRAM Inc. notified Phyne Pharmaceuticals that AMRAM Inc. was
recalling these products because they were manufactured under sub-standard conditions.
FDA is issuing today's warning because Phyne Pharmaceuticals has delayed taking prompt
and appropriate action to remove these products from the market.
The nationwide recall follows FDA's recent inspections of Phyne Pharmaceuticals and
AMRAM Inc. During the inspections, FDA found violations of requirements for good
manufacturing standards for pharmaceuticals. These requirements help ensure that drug
products are safe and effective. The violations FDA found demonstrate that the products
lack assurance of sterility and potency.
Anyone in possession of these products is urged to contact and to return the products
to Phyne Pharmaceuticals at 7950 East Red Field Rd., Scottsdale, Ariz. 85267, (800)
345-3391 or 480-998-4142, FAX (480) 443-4775. Phyne Pharmaceuticals has stated they will
be providing specific return instructions to their customers by an "Urgent Voluntary
Drug Recall" letter dated January 25, 2001.
The following is the most up-to-date list of products under recall by Phyne
Pharmaceuticals. Some of the products are labeled with both AMRAM, Inc. and Phyne
Pharamceuticals; however, some may bear one or the other company's name as the
manufacturer and/or distributor with or without the other company's name listed.
All lot numbers and codes, strengths and sizes and expiration dates of the following
injectable products are included in this recall:
- Adenosine Monophosphate
- Ascorbic Acid Injection
- Beet Ascorbic Acid Injection
- Biotin
- Colchicine
- Vitamin B-12(Cyanocobolamin)
- Dexpanthenol
- Disol, USP Brand of EDTA
- Echinacea Homeopathic Injection
- Edetate Disodium
- Endocrine
- Adrenal Cortex Extract (ACE)
- Folic Acid
- Germanium Sesg.(Sesguloxide)
- L-Glutathione or Glutathione
- Human Chorionic Gonadotropin
- Hydrochloric Acid
- Iron 59 Injection
- Liver Injection, Crude
- Lypo-Vite Injection
- Magnesium Chloride Injection
- M.I.C.
- Procaine Hydrochloride Injection
- Pyridoxine HCL (B-6)
- Sodium Thiosalicylate
- Superoxide Dismutase (S.O.D.)
- L-Taurine Injection
- Thiamine HCL
- Thymus Extract
- Choline Chloride
- Diphenhydramine
- Glycyrrhizen
- Chlorpheniramine Injection
- Hydrogen Peroxide
- Hydroxocobalamin
- MIC with Folic Acid
- Niacin
- Pangamic Acid
- Riboflavin
Patients who believe they might have been injured by these products should immediately
consult with their health care provider. FDA is aware of three serious injuries associated
with the use of one of the recalled products, Colchicine, labeled as containing .5mg/ml
but actually formulated at a concentration of 5mg/ml.
Any adverse reactions experienced with the use of these products should also be
reported to the FDA's MEDWATCH Program by phone at 1-800-FDA-1088, by fax at
1-800-FDA-0178, by mail at MEDWATCH, HF-2, FDA 5600 Fishers Lane, Rockville, MD
20852-9787, or on the MEDWATCH web site at www.fda.gov/medwatch.
USFDA ANNOUNCES WARNING TO PREGNANT &
PREGNANT TO BE WOMEN ON METHYL MERCURY IN FISH
The Food and Drug Administration (FDA) is announcing its advice to pregnant women and
women of childbearing age who may become pregnant on the hazard of consuming certain kinds
of fish that may contain high levels of methyl mercury. The FDA is advising these women
not to eat shark, swordfish, king mackerel, and tilefish. As a matter of prudent public
health advice, the FDA is also recommending that nursing mothers and young children not
eat these fish as well.
Fish such as shark, swordfish, king mackerel, and tilefish contain high levels of a
form of mercury called methyl mercury that may harm an unborn baby's developing nervous
system. These long-lived, larger fish that feed on smaller fish accumulate the highest
levels of methyl mercury and therefore pose the greatest risk to the unborn child. Mercury
can occur naturally in the environment and it can be released into the air through
industrial pollution and can get into both fresh and salt water.
The FDA advisory acknowledges that seafood can be an important part of a balanced diet
for pregnant women and those of childbearing age who may become pregnant. FDA advises
these women to select a variety of other kinds of fish -- including shellfish, canned
fish, smaller ocean fish or farm-raised fish -- and that these women can safely eat 12
ounces per week of cooked fish. A typical serving size of fish is from 3 to 6 ounces.
The FDA's Center for Food Safety and Applied Nutrition will launch a comprehensive
education program to reach pregnant women and women of childbearing age who may become
pregnant and their health care providers concerning the hazard posed by methyl mercury to
the unborn child. As one of its priorities for fiscal year 2001, the Center will also
develop our overall public health strategy for future regulation of methyl mercury in
commercial seafood.
Today, EPA is also issuing advice on possible mercury contamination to women and
children eating fish caught by family and friends (non-commercial fish). EPA particularly
recommends that consumers check with their state or local health department for any
additional advice on the safety of fish from nearby waters. Additional information is
available on EPA's Web site at: http://www.epa.gov/ost/fish.
HERBAL CARCINOGEN AND CO-CARCINOGENIC DEATH DRUG
IDENTIFIED AND RECALLED
BMK International Voluntarily Recalls Neo Concept Aller Relief Because of Possible
Health Risk
WELLESLEY, MA - January 19, 2001 - BMK International is voluntarily recalling Neo
Concept Aller Relief after receiving notification from the FDA that the product contains
trace amounts of aristolochic acid. Aristolochic acid is a potent carcinogen and
nephrotoxin found in certain plants and botanicals. Products that contain arstolochic acid
have been associated with several occurrences of kidney failure in Europe. The use of
aristolochic acid containing products has also been linked to the increase risk of kidney
cancer in people who have consumed it.
Aller Relief was distributed nationwide to licensed health care practitioners, and
retail outlets. Aller Relief is packaged in 30-ct. and 90-.ct. capsules. The lot numbers
covered in this recall are 30-ct. and 90-ct.: #003480, #0006480.
No complaints or reports illnesses have been reported to date.
The recall is a result of the FDA notification that recommended manufacturers test
their products that contain herbs that may be contaminated with aristolochic acid. The
company was informed by the FDA that the product contains trace amounts of aristolochic
acid and thus is conducting a voluntary recall. The company has reformulated the Aller
Relief product to ensure that in the future no herb in the formula contains or may be
adulterated with aristolochic acid. The reformulated product will available shortly.
Consumers with questions can call telephone: (781) 235-9999. Consumers should return
the product to the place of purchase for a full cash refund. (Editor's note:
November 21, 2000, East Earth Herb recalled Jade Pharmacy Brand "Meridian Circulation
and Quell Fire" do to similar patient catastrophes.)
CDC ANNOUNCES NEW YOUTH VIOLENCE PREVENTION
WEBSITE
CDC's National Center for Injury Prevention and Control announced today the launch of a
new web-based resource for people interested in learning more about preventing youth
violence and suicide. The National Youth Violence Prevention Resource Center will serve as
a central source for prevention information gathered from institutions, community-based
organizations and federal agencies.
The Resource Center, designed and developed in partnership with the White House Council
on Youth Violence, features a Web site, a toll-free hotline, and a fax-on-demand service.
It offers access to information about prevention programs, publications, research and
statistics, fact sheets and more.
"In 1998, more than 3,400 people under 19 years old died from violence-related
injuries. As a result, we find that parents, teachers, students, researchers and many
others are becoming increasingly involved in identifying ways to reduce the spread of
violence in their communities. We believe the Resource Center will give them the
information they need to do that more effectively," said Rodney Hammond, Ph. D.,
director of the Division of Violence Prevention for the National Center for Injury
Prevention and Control.
The Resource Center's web site is www.safeyouth.org.
In addition to serving the needs of public health professionals, the site includes
separate sections for parents and teens. The hotline is available Monday through Friday, 8
a.m. to 6 p.m. EST, by calling 1-866-SAFEYOUTH (1-866-723-3968.) Fax-on-demand
service is available at all times.
The Centers for Disease Control and Prevention (CDC) protects people's health and
safety by preventing and controlling diseases and injuries; enhances health decisions by
providing credible information on critical health issues; and promotes healthy living
through strong partnerships with local, national and international organizations.
FTC SETTLES FALSE RESULTS HIV CASE
Two manufacturers of Food and Drug Administration unapproved rapid HIV tests have
settled Federal Trade Commission charges that, in some instances, their tests did not
accurately detect the presence of HIV antibodies. Under the terms of the settlements,
Chembio Diagnostic Systems, Inc. and Alfa Scientific Designs, Inc. will be barred from
making, or assisting others in making, any false or misleading representations concerning
the accuracy of any unapproved HIV test or other unapproved device. The two settlements
are the latest in a series of FTC enforcement actions against marketers of unapproved
rapid HIV tests, and the first cases against manufacturers of the devices.
Chembio is based in Medford, New York. Alfa is headquartered in San Diego, California.
In its complaint against Chembio, filed in the Eastern District of New York last week,
the Commission alleged that the company represented that its tests were more than 99
percent accurate in detecting the presence of HIV antibodies in human blood, serum or
plasma. According to Commission allegations, however, Chembio's tests failed to detect the
presence of HIV in some instances.
Under the stipulated final order settling the charges, Chembio is prohibited from
making false or misleading representations in connection with the advertising or sale of
any HIV test, or any other medical device not approved by the U.S. Food and Drug
Administration, including any claims regarding the accuracy of the tests. The settlement
also requires the defendant to notify the Commission of any complaints or refund requests
in the future and allows the Commission, for a period of five years, to randomly select
and test any HIV test or other unapproved device for accuracy.
In a separate matter, the Commission settled its lawsuit against Alfa Scientific, and
amended its complaint to name as additional defendants Alfa Scientific's President, Naishu
Wang, M.D., Ph.D., and the company's Chief Executive Officer, David F. H. Zhou, M.D.,
Ph.D. The Commission alleged in its amended complaint that Alfa, Wang and Zhou violated
federal law when they represented on their Internet site that their "Alfa HIV-1/2
Rapid Tests" accurately detected HIV infection in human blood. According to the FTC,
independent tests showed that Alfa's HIV tests produced false negative results when tested
with HIV-positive whole blood samples.
The settlement prohibits Alfa, Wang and Zhou from making false or misleading
representations in connection with the advertising or sale of any HIV test, or any other
medical device not approved by the U.S. Food and Drug Administration, including any claims
regarding the accuracy of the tests. The settlement also requires the defendants to notify
the Commission of any complaints or refund requests in the future and allows the
Commission, for a period of five years, to randomly select and test any HIV test or other
unapproved device for accuracy.
In November 1999, the FTC settled similar charges against Cyberlinx Marketing, Inc.,
and its President, Jeffrey S. Stein, of Las Vegas, Nevada. Cyberlinx had obtained its
rapid HIV tests from a San Francisco distributor, Sovo Tec Diagnostic Designs, Inc. Sovo
Tec, which settled similar charges with the FTC last September, had purchased its HIV
tests from Chembio, the subject of one of the actions announced by the Commission today.
In March 2000, the Commission settled another case against a Florida distributor of
rapid HIV tests, David M. Rothbart, President of Medimax, Inc. According to the FTC, Alfa
manufactured the HIV tests distributed by Medimax.
Rapid HIV tests use a simple finger prick process for blood collection or a special
sponge device for saliva collection. The sample is applied to a plastic testing device and
a developing solution, or diluent, is added to determine if the sample is positive for
antibodies to HIV. Results are generally available in fifteen minutes. Currently, just one
rapid HIV test is approved for sale in the U.S. and is available only to medical
professionals. The rapid HIV tests both Alfa and Chembio manufactured and distributed
cannot be sold in the United States but under federal law can be exported without FDA
approval. Most unapproved rapid HIV tests are distributed in developing nations. In
November 1999, the FTC and FDA issued a joint statement warning consumers that unapproved
HIV tests can give inaccurate results.
The Commission votes to approve the settlements were 5-0, with Commissioner Orson
Swindle issuing a separate statement.
Commissioner Swindle issued a statement praising both settlements as "a tremendous
public service," but cautioned that "enforcement of the FTC Act cannot
systematically address the export from the United States of potentially faulty HIV
tests." Referring to his statement in a related case, Sovo Tec Diagnostics, Inc.,
in which he raised questions about the treatment under current U.S. law of exports of
unapproved rapid HIV tests, Swindle expressed concern that "there may be
unanticipated gaps . . . that allow the export of some U.S.-manufactured HIV tests and
test kits without independent scrutiny of their effectiveness, whether by the FDA or by a
foreign government that authorizes the marketing of such devices. A system designed to
prevent wasteful, duplicative review may have led to the unintended consequence of
ineffective review." He urged the FDA and Congress to "take a hard look at the
export regime to be sure that it is not inadvertently undermining U.S. and international
efforts to combat the AIDS pandemic."
LASIK is a
surgical procedure intended to reduce a person's dependency on glasses or contact lenses.
The goal of this Web site is to provide objective information to the public about LASIK
surgery. See other sections of this site to learn about what you should know before surgery, what will happen during the surgery, and what
you should expect after
surgery. There is a glossary of
terms and a checklist of issues for
you to consider, practices to follow, and questions to ask your doctor before undergoing
LASIK surgery.
LASIK stands for
Laser-Assisted In Situ Keratomileusis and is a procedure that permanently
changes the shape of the cornea, the clear covering of the front of the eye, using an
excimer laser. A knife, called a microkeratome, is used to cut a flap in the
cornea. A hinge is left at one end of this flap. The flap is folded back revealing the
stroma, the middlesection of the cornea. Pulses from a computer-controlled laser vaporize
a portion of the stroma and the flap is replaced.
FDA PROPOSES NEW RULES FOR "GOOD TISSUE
PRACTICE"
FDA today proposed a new regulation on current good tissue practice (GTP), which
includes the methods, facilities and controls used for the manufacture of human cellular
and tissue-based products. This proposed rule is the last of three proposals designed to
implement FDA’s 1997 “Proposed Approach to the Regulation of Cellular and
Tissue-based Products”, a comprehensive risk-based regulatory framework designed to
help ensure the safety and quality of products, including new technologies, without
imposing unnecessary regulatory requirements.
The purpose of the GTP regulations is to help ensure that donors of human cellular and
tissue-based products are free of communicable diseases, and that the cells and tissues
are not contaminated during manufacturing and maintain their integrity and function. Key
elements of the proposed rule are:
- Establishment of a quality program, which would evaluate all aspects of the firm’s
operations, to ensure compliance with GTP;
- Maintenance of an adequate organizational structure and sufficient personnel;
- Establishment of standard operating procedures for all significant steps in
manufacturing;
- Maintenance of facilities, equipment and the environment;
- Control and validation of manufacturing processes;
- Provisions for adequate and appropriate storage;
- Record keeping and management;
- Maintenance of a complaint file;
- Procedures for tracking the product from donor to recipient, and from recipient to
donor.
These fundamental, base-line regulations would apply to manufacturers of all human
cellular and tissue-based products. In addition, all of these manufacturers would be
required to report adverse reactions and certain product deviations, have adequate
labeling that is not false or misleading and allow FDA inspections to ensure compliance
with regulations. Certain cellular and tissue-based products that require licensing or
premarket approval as biological products or medical devices would be subject to more
comprehensive requirements based on their risks.
Two other related proposed rules to implement the 1997 regulatory approach to tissues
and cells have already been published. The first one was (“Establishment Registration and
Listing for Manufacturers of Human Cellular and Tissue-Based Products”) published
May 14, 1998 and required tissue facilities to register with the FDA and list their
products. This proposed rule is currently undergoing review and is expected to be
published in final form soon. The other one, (“Suitability Determination for Donors of
Human Cellular and Tissue-Based Products”) issued on Sept 30, 1999, focuses on
donor screening and testing measures to prevent the unwitting use of contaminated tissues
with potential to transmit infectious diseases.
FDA’s current regulations addressing tissues were promulgated in December 1993
with an interim final rule that required the screening and testing of tissue donors for
certain transmissible diseases such as HIV and hepatitis, as well as the screening of
donors for behavioral risk factors. The final rule, which was published
on July 29, 1997, became effective on January 26, 1998. The new proposed rules are more
comprehensive and include provisions for the regulation of innovative products.
CUSTOMER SATISFACTION RESULTS FOR THE FOOD AND
DRUG ADMINISTRATION REMAIN CONSTANT
The results of the second government-wide customer satisfaction survey released today
show that consumers continue to be satisfied with the FDA's performance in food labeling
and consumer alerts on food safety issues, and continue to have confidence and trust in
the FDA to ensure food safety for consumers.
This survey, initiated last year by the National Partnership for Reinventing
Government, was developed to measure how well key government agencies serve the American
public and set a baseline for measuring customer satisfaction with the Federal government.
The survey was conducted by the University of Michigan using a model established for
the American Customer Satisfaction Index, which measures satisfaction with various
industries. The FDA received an index score of 68 in the customer survey, which is two
points higher than last year's score, but is not a statistically significant change.
Customers were randomly selected and asked about their expectation and the quality of
the services or products they received from the various agencies. Principal grocery
shoppers and food preparers were interviewed for the FDA survey. Survey questions asked
about the mission of the FDA to ensure food safety; the usefulness and clarity of
nutrition labeling, customer awareness, and the views on effectiveness of inspecting,
testing and labeling efforts.
In addition, similar questions were asked about meat and poultry products regulated by
the U.S. Department of Agriculture (USDA). In addition to the positive responses about
nutrition labeling and food safety, those surveyed were concerned about the timeliness of
consumer alerts and had less awareness of the FDA's mission in food safety. The survey
results, as in the 1999 report, call for efforts to increase in public awareness on how
FDA food safety activities affect the consumer.
"The nutrition label has made it easier for Americans to make informed food
choices," said Jane E. Henney, M.D., Commissioner of the Food and Drug
Administration. "Food safety has been a top priority for the FDA as a part of the
Food Safety Initiative and the public depends on the FDA to continue to build on its
successes in protecting the public health, especially with egg, seafood, and produce
safety."
The FDA has undertaken a number of activities in the area of labeling and food safety
this year. A new web site on using the nutrition facts panel of the food label was
initiated this fall and can be accessed at
http://vm.cfsan.fda.gov/~dms/foodlab.html In the arena of food safety, the agency has
issued regulations on egg safety labeling and refrigeration; has approved the use of
irradiation to reduce pathogen on sprout seeds, shell eggs and juice, and has completed an
evaluation of the Seafood HACCP program. The agency is preparing draft risk assessments
for the pathogens Listeria monocytogenes and Vibrio parahaemolyticus and is
issuing regulations for food produced with biotechnology and dietary supplement good
manufacturing practices. As well as posting FDA recall information on its web site, the
FDA now includes press releases of voluntary recalls issued by manufacturers, so consumers
will have this information in a timely manner.
The agency continues to support a wide range of outreach activities including its
website (www.fda.gov), the FDA information
line (1-888-INFO-FDA), and the Center for Food Safety and Applied Nutrition information
line (1-888-SAFEFOOD). The FDA also continues to support the "Fight BAC"
campaign a collaborative program involving government, industry, academia, and consumer
groups which focuses on consumer education about safe food handling. One example of this
outreach is the FDA-National Science Teachers Association Food Science Professional
Development Program designed to assist middle and high school teachers in working food
science into their science curriculums.
LEADING
CAUSES OF DEATH
(All figures are for U.S.)
 Ten Leading Causes
of Death in the U.S.: (1998) Ten Leading Causes
of Death in the U.S.: (1998)
 Heart Disease: 724,859 Heart Disease: 724,859
Cancer: 541,532
Stroke: 158,448
Chronic Obstructive Pulmonary Disease: 112,584
Accidents: 97,835
Pneumonia/Influenza: 91,871
Diabetes: 64,751
Suicide: 30,575
Nephritis, nephrotic syndrome, and nephrosis: 26,182
Chronic Liver Disease and Cirrhosis: 25,192
Source: National Vital Statistics Reports, Vol. 48, No. 11
Comprehensive Data
Ten Leading Causes of Death, by Sex, Race, and Age
View/download PDF
Ten Leading Causes of Death Among Hispanics, by Sex and Age
View/download PDF
Selected Leading Causes of Death in 50 States
View/download PDF
PHYSICIAN LABELING PROPOSAL
The Food and Drug Administration today proposed a new format for prescription drug
labeling that will help reduce medical errors, which according to the National Academy of
Sciences may be responsible for as many as 98,000 U.S. deaths annually. FDA believes that
this new, user- friendly format will reduce errors in drug prescribing.
"Today's proposal is FDA's latest initiative to improve the labeling of the
products it regulates," said Dr. Jane E. Henney, FDA Commissioner. "This
proposal is particularly valuable because it will make important information available in
a clear, consistent, and readable format that is essential to proper prescribing
practices."
Prescription drug product labeling, also known as the package insert, represents a
primary means of providing critical information about drugs to practitioners. As part of
the drug review process, FDA reviews and approves drug product labeling that is initially
proposed by manufacturers.
An FDA study showed that practitioners found drug product labeling to be lengthy,
complex, and hard to use. The proposed new format would provide user-friendly labeling
that would allow practitioners to quickly find the most important information about the
product. One major change is inclusion of a new introductory "Highlights"
section of bulleted prescribing information. This section would include the information
that practitioners most commonly refer to and view as most important, and it would provide
the location of further details elsewhere in the labeling.
The proposed new labeling is expected to reduce practitioners' time spent looking for
information, decrease the number of preventable medical errors, and improve treatment
effectiveness. The information will be easier to find, read and use, and it should also
enhance the safe and effective use of prescription drugs and reduce medical errors caused
by inadequate communication. Because these labeling revisions represent considerable
effort and are most critical for newer and less familiar drugs, the proposal will apply
only to relatively new prescription drug products.
For further information,
see the Federal Register for Dec. 21, 2000.
FDA APPROVES NEW TREATMENT FOR ECZEMA
The Food and Drug Administration (FDA) today approved a new treatment for atopic
dermatitis (eczema) - a non-contagious skin condition that can cause redness, itching and
oozing lesions.
The drug is Protopic (tacrolimus) Ointment (0.1% and 0.03% for adults and 0.03% for
children 2 years and older). The drug is for patients with moderate to severe eczema, for
whom standard eczema therapies are deemed inadvisable because of potential risks, or who
are not adequately treated by or who are intolerant of standard eczema therapies.
FDA based its approval on the results of three 12- week studies which indicated that
28-37% of patients using Protopic experienced greater than or equal to 90% improvement of
their skin condition, as measured by physicians, and two one year studies that indicated
that the drug is safe for intermittent long term use.
Common side effects associated with this drug include temporary stinging or burning
sensations where the drug is applied, which may lessen if the diseased skin heals. There
was evidence from an animal study that Protopic Ointment may accentuate the adverse
effects of ultraviolet light on the skin. Therefore, it is important that patients avoid
sunlight and sun lamps, tanning beds, and treatment with UVA or UVB light. Patients who
need to be outdoors after applying Protopic should wear loose fitting clothing that
protects the treated area from the sun. In addition, patients should ask their health care
providers what other type of protection from the sun to use.
The drug should not be used by patients who are allergic to its active ingredient,
tacrolimus, or to its inactive ingredients. Women who are breastfeeding should also avoid
using this drug. Women who are pregnant or who are planning to become pregnant should
check with their physicians before using this product.
Unpowered Scooter-Related Injuries --- United States,
1998--2000
Injuries associated with unpowered scooters have increased dramatically since May 2000
(1). These scooters are a new version of the foot-propelled scooters first popular
during the 1950s. Most scooters are made of lightweight aluminum with small, low-friction
wheels similar to those on in-line skates. They weigh <10 pounds and fold for easy
portability and storage. Up to 5 million scooters are expected to be sold in 2000, an
increase from virtually zero last year (Consumer Product Safety Commission [CPSC],
unpublished data, 2000). This report summarizes the results of a descriptive analysis
of scooter-related injuries during the past 34 months and provides recommendations to
reduce these injuries.
CPSC and CDC analyzed preliminary data from CPSC's National Electronic Injury
Surveillance System (NEISS) from January 1998 through October 2000 and the Injury
and Potential Injury Incident File (IPII) during January--October 2000. NEISS is a
probability sample of 100 U.S. hospitals with 24-hour emergency departments (EDs) and more
than six beds. NEISS collects data from these hospitals on all persons seeking treatment
for consumer product-related injury in the hospitals' EDs. Estimates of injuries in the
United States associated with specific consumer products or activities can be made from
NEISS data. Data were weighted according to the probability of hospital selection in the
NEISS sample to provide estimates for the U.S. population (2). IPII consists of
anecdotal information reported to CPSC from many sources (e.g., coroners and medical
examiners; newspaper reports; consumer complaints through the CPSC hotline or CPSC's
World-Wide Web site; and referrals from federal, state, and local officials). NEISS
was used to estimate scooter-related injuries, and IPII was used to identify
scooter-related deaths. Because the new scooters were introduced in large numbers into the
United States market in 2000, the 1998 and 1999 data relate to the older versions of
scooters.
During January--October 2000, an estimated 27,600* (95% confidence limits
[CL]=22,190--33,010) persons sought ED care for scooter-related injuries. In
August, September, and October 2000, the estimated number of injuries requiring ED care
was 6,529 (95% CL=4,610--8,450), 8,628 (95% CL=6,090--11,170), and 7,359 (95%
CL=5,200--9,520), respectively (Figure 1); October data are incomplete
and may change slightly as additional injury reports are filed. The estimated number of
injuries during August--October represents 80% of the estimated total number of injuries
for all of 2000. Each of the preceding 3 months also exceeded the 12-month total for
either 1998 or 1999. The estimated number of injuries seen in EDs in September 2000 was
nearly 18 times higher than in May 2000.
Approximately 85% of persons treated in EDs were children aged <15 years, and 23%
were aged <8 years; two thirds were male. The most common type of injury was a fracture
or dislocation (29%), of which 70% were to the arm or hand. Other injuries included
lacerations (24%), contusions/abrasions (22%), and strains/sprains (14%). Forty-two
percent of all injuries occurred to the arm and hand, 27% to the head and face, and 24% to
the leg and foot.
Two persons have died while using a scooter. An adult fell and struck his head while
showing his daughter how to ride the scooter. A 6-year-old boy rode into traffic and was
struck by a car.
Reported by: GW Rutherford, Jr, MS, R Ingle, MA, Consumer Product Safety Commission.
Div of Unintentional Injury Prevention, National Center for Injury Prevention and Control,
CDC.
CDC Editorial Note:
The findings in this report demonstrate the rapid increase in injuries associated with
riding the new lightweight, folding, unpowered scooters, which are a fast-growing activity
in the United States. Because these scooters are a recent phenomenon, scientific
data about the efficacy of safety equipment to protect against scooter-related injuries
are not available. However, lessons learned from similar recreational activities (e.g.,
in-line skating) can guide users in adopting reasonable safety precautions, such as
wearing protective gear.
On the basis of data from in-line skating and bicycling, many of these injuries might
have been prevented or reduced in severity had protective equipment been worn. Helmets can
prevent 85% of head injuries (3), elbow pads can prevent 82% of elbow injuries, and
knee pads can prevent 32% of knee injuries (4). Although wrist guards are effective
in preventing injuries among in-line skaters, the protection they provide against injury
for scooter riders is unknown because wrist guards may make it difficult to grip the
scooter handle and steer it.
The public health community can be proactive and support efforts to decrease
scooter-related injury in children by increasing awareness among parents and health-care
providers of the injury potential and the need for safety measures when using scooters.
Many children may not be prepared developmentally to handle the multitask challenges they
may experience while riding a scooter. Changes in the product and rider behavior also may
make riding scooters safer. The mechanisms and circumstances of scooter-related injury
require further research.
On the basis of evidence of injury prevention effectiveness for other related
activities, the following recommendations may help prevent scooter-related injuries:
- Wear a helmet that meets the standard established by CPSC;
- Use knee and elbow pads;
- Ride scooters on smooth, paved surfaces without traffic, and avoid streets and surfaces
with water, sand, gravel or dirt;
- Do not ride scooters at night; and
- Young children should not use scooters without close supervision.
References
- Consumer Product Safety Commission. National Electronic Injury Surveillance System
[computer file]. Washington, DC: Consumer Product Safety Commission, November, 2000.
- Kessler E, Schroeder T. The NEISS sample (design and implementation). Washington, DC:
Consumer Product Safety Commission, October 1998.
- Thompson RS, Rivara FP, Thompson DC. A case-control study of the effectiveness of
bicycle safety helmets. N Engl J Med 1989;320:1361--7.
- Schieber RA, Branche-Dorsey CM, Ryan GW, Rutherford GW, Stevens JA, O'Neil J. Risk
factors for injuries from in-line skating and the effectiveness of safety gear. N Engl J
Med 1996;335:1630--5.
* Estimates are based on the approximate range at the 95% confidence level of
relative sampling error. For this analysis, the corresponding relative sampling error for
the estimated number of injuries during January--October is 0.1.
-Article written by CDC
|

 Beat the Press
Beat the Press


 FOR JUSTICE THROUGH SCIENCE ONLY:
FOR JUSTICE THROUGH SCIENCE ONLY: